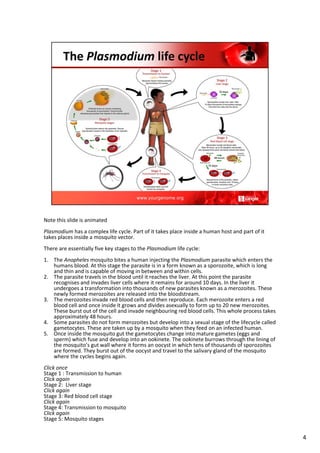
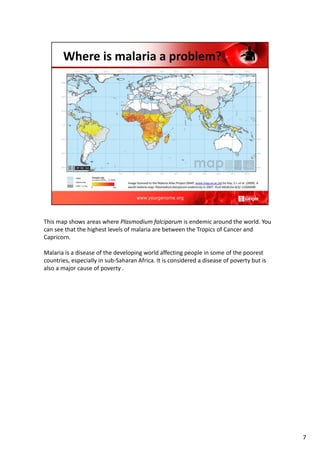
Malaria is an infectious disease spread by mosquitoes that infects over 3 billion people worldwide. It is caused by a parasite called Plasmodium, which has a complex life cycle involving both human and mosquito hosts. Young children and pregnant women are most vulnerable. While rates of malaria have decreased, it remains a major public health problem and cause of economic hardship in developing countries. Controlling mosquitoes and proper diagnosis/treatment of infections are key to reducing the malaria burden.