Download to read offline
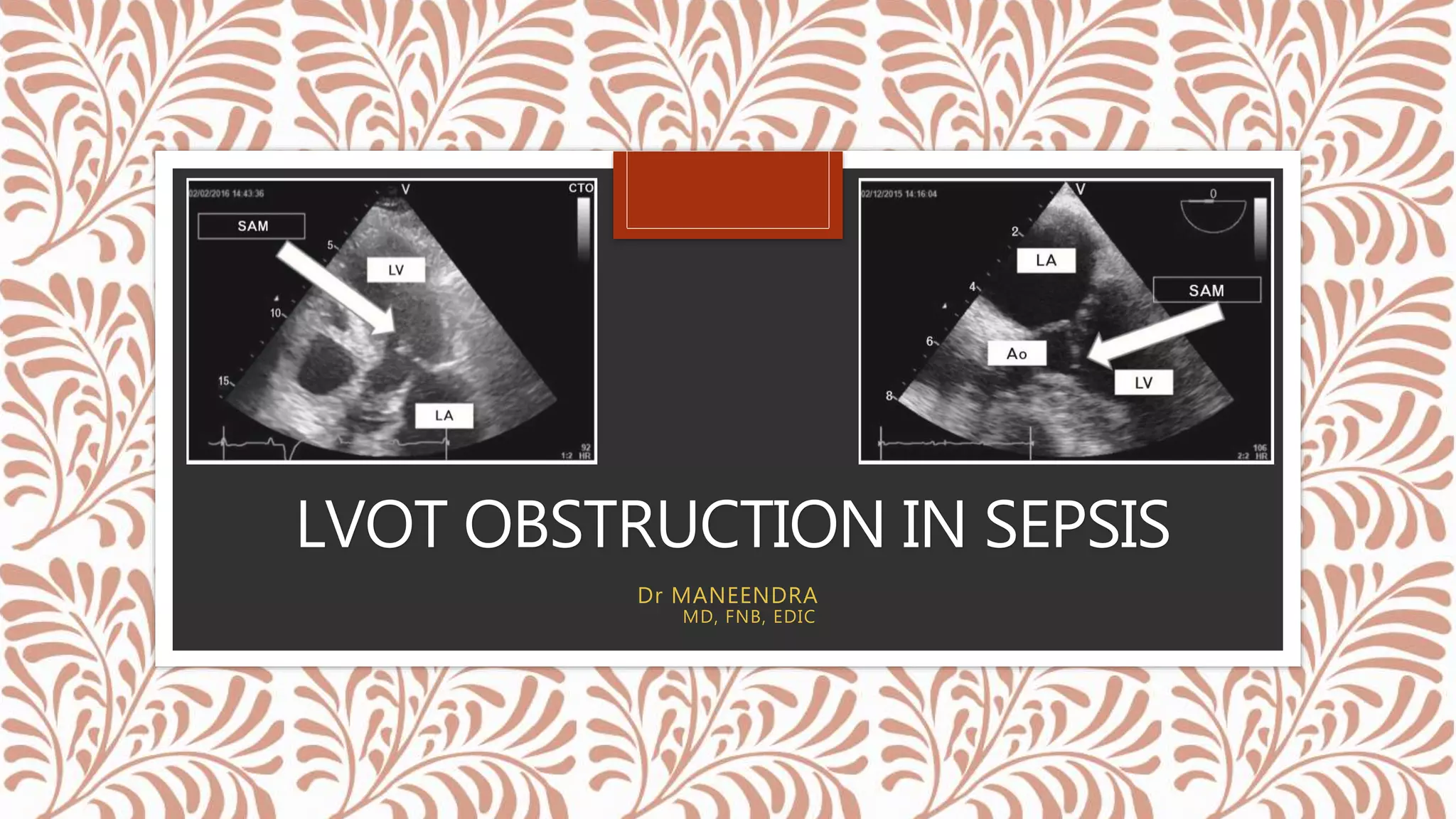
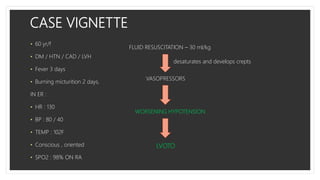
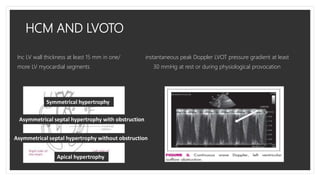
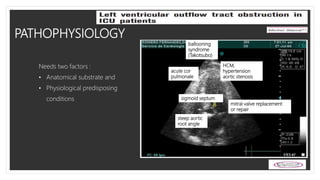
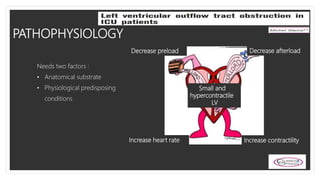
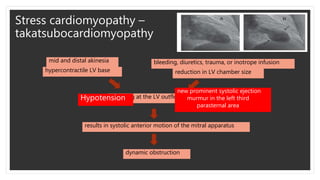
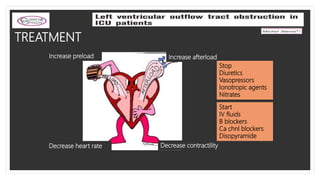
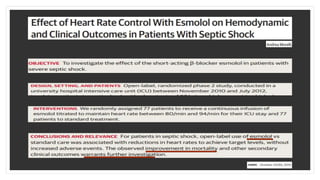
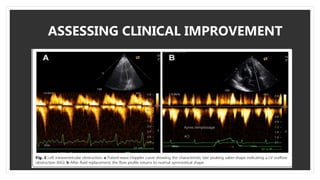
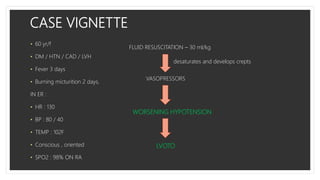

This document discusses a case of left ventricular outflow tract (LVOT) obstruction in a septic 60-year-old female patient. LVOT obstruction can occur when there is an anatomical substrate like hypertrophic cardiomyopathy combined with physiological stressors like sepsis that decrease preload and increase contractility. The patient's hypotension worsened due to the LVOT obstruction. Echocardiogram is needed to diagnose and treatment involves increasing preload, decreasing contractility, and using beta-blockers and calcium channel blockers. The importance of recognizing LVOT obstruction in sepsis is discussed as well as prospectively studying the gradient and how it relates to treatment response and mortality.