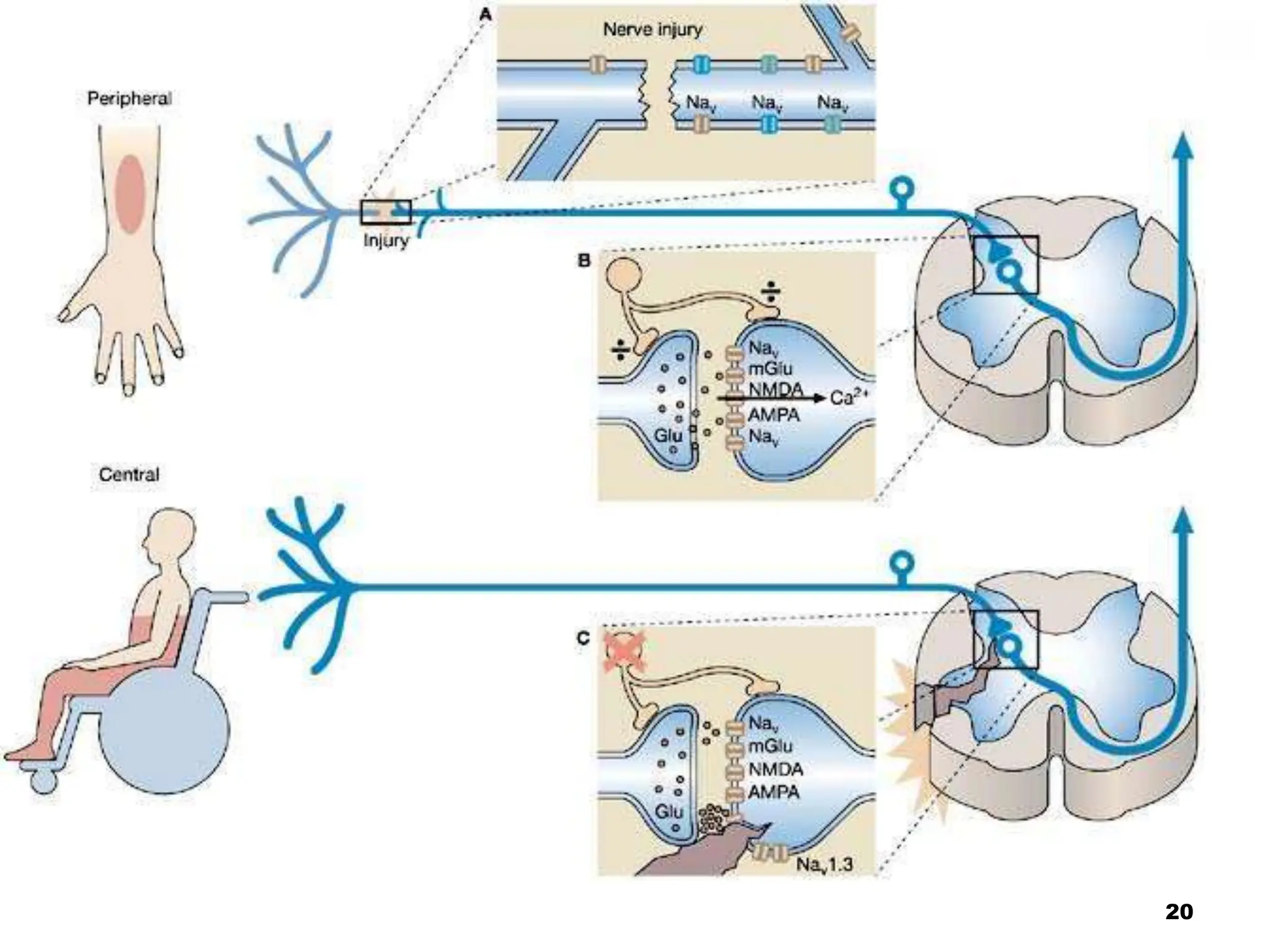
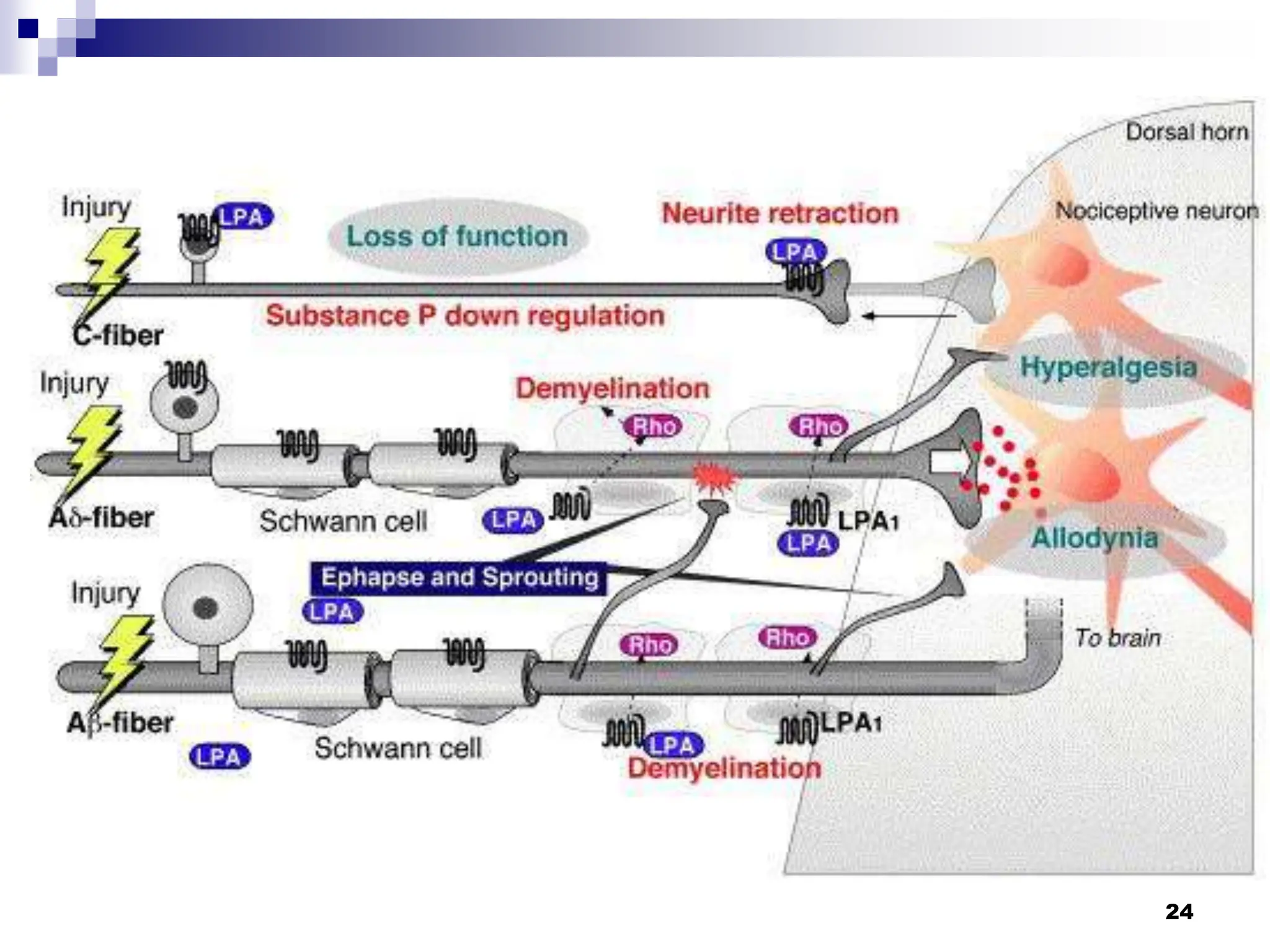
This document discusses orofacial pain and neuropathic pain. It provides information on differential diagnoses for orofacial pain and summarizes a study on oral and maxillofacial surgery in patients with chronic orofacial pain. The document also discusses the challenges in diagnosing and treating neuropathic pain, highlighting evidence that neuropathic pain results from complex peripheral and central mechanisms in the nervous system.