Download to read offline

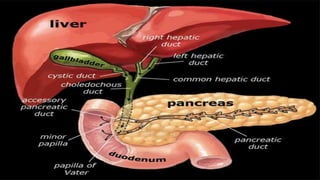
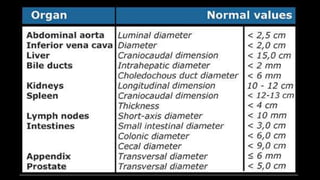
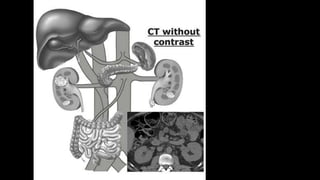
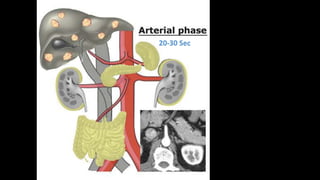
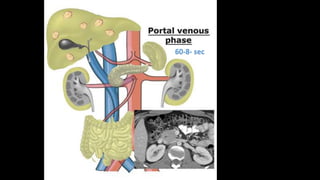
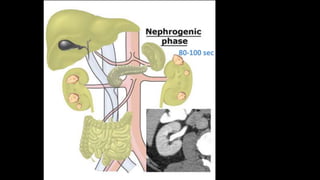
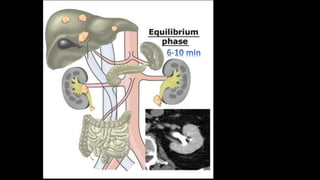

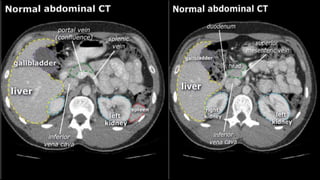
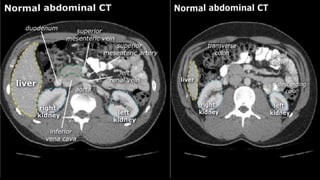
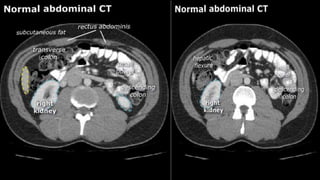
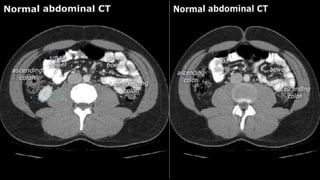
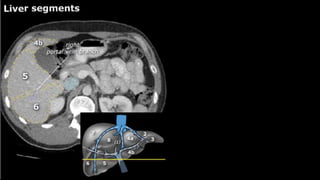
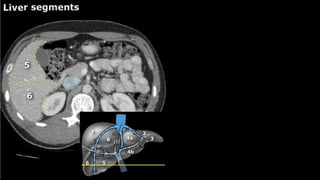
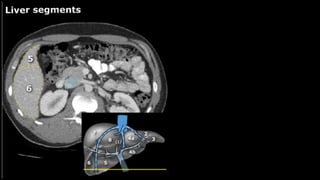
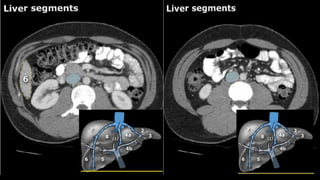
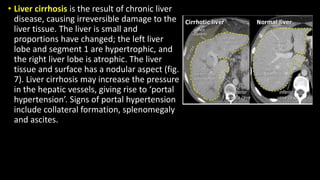
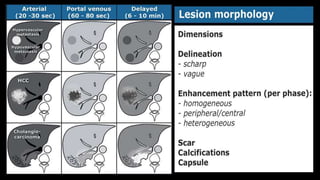
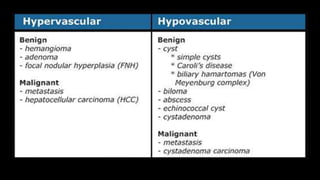

This document provides an overview of normal liver anatomy and imaging characteristics, as well as common liver lesions. It describes that the liver normally enhances homogeneously in all phases. Common benign liver lesions include cysts, hemangiomas and focal nodular hyperplasia. Malignant lesions discussed are hepatocellular carcinoma and cholangiocarcinoma. Cirrhosis causes an atrophic right lobe and hypertrophic left lobe. The gallbladder and bile ducts are also reviewed.



































































