Lipoproteins metabolism for MMBS, Lab. Med. BDSpptx
•Download as PPTX, PDF•
1 like•68 views

Lipids are insoluble in water, the problem of transportation in the aqueous plasma is solved by associating nonpolar lipids (triacylglycerols and cholesteryl esters) with amphipathic lipids (phospholipids and cholesterol) and proteins to make water-miscible lipoproteins.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Lipoproteins metabolism for MMBS, Lab. Med. BDSpptx
Similar to Lipoproteins metabolism for MMBS, Lab. Med. BDSpptx (20)
More from Rajendra Dev Bhatt
More from Rajendra Dev Bhatt (20)
Recently uploaded
Recently uploaded (20)
Lipoproteins metabolism for MMBS, Lab. Med. BDSpptx
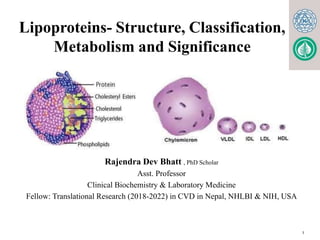
- 1. Lipoproteins- Structure, Classification, Metabolism and Significance 1 Rajendra Dev Bhatt , PhD Scholar Asst. Professor Clinical Biochemistry & Laboratory Medicine Fellow: Translational Research (2018-2022) in CVD in Nepal, NHLBI & NIH, USA
- 2. Lipids absorbed from the diet and synthesized by the liver and adipose tissue must be transported between various cells and organs for utilization and storage. Lipids are insoluble in water, the problem of transportation in the aqueous plasma is solved by associating nonpolar lipids (triacylglycerols and cholesteryl esters) with amphipathic lipids (phospholipids and cholesterol) and proteins to make water-miscible lipoproteins. Lipoproteins:
- 3. General Structure of Lipo proteins Lipoproteins consist of a nonpolar core and a single surface layer of amphipathic lipids Th e nonpolar lipid core consists of mainly triacylglycerol and cholesteryl ester and is surrounded by a single surface layer of amphipathic phospholipid and cholesterol molecules These are oriented so that their polar groups face outward to the aqueous medium. The protein moiety of a lipoprotein is known as an apolipoprotein or apoprotein.
- 4. General Structure of Lipo proteins Some apolipoproteins are integral and cannot be removed, whereas others can be freely transferred to other lipoproteins.
- 5. Classification of Lipoproteins Lipoproteins can be classified in three ways- 1) Based on density- They are separated by Ultracentrifugation. Five major groups of lipoproteins have been identified that are important physiologically and in clinical diagnosis. (i) Chylomicons, derived from intestinal absorption of triacylglycerol and other lipids; Density is generally less than 0.95 while the mean diameter lies between 100- 500 nm
- 6. Classification of Lipoproteins 1) Based on density (contd.) (ii) Very low density lipoproteins (VLDL), derived from the liver for the export of triacylglycerol; density lies between 0.95- 1.006 and the mean diameter lies between 30-80 nm. (iii)Intermediate density lipoproteins (IDL) are derived from the catabolism of VLDL,with a density ranging intermediate between Very low density and Low density lipoproteins i.e. ranging between 1.006- 1.019 and the mean diameter ranges between 25- 50nm.
- 7. Classification of Lipoproteins Based on density (contd.) iv) Low-density lipoproteins (LDL), representing a final stage in the catabolism of VLDL; density lies between 1.019-1.063 and mean diameter lies between 18-28 nm (iv) High-density lipoproteins (HDL), involved in cholesterol transport and also in VLDL and chylomicron metabolism. Density ranges between 1.063-1.121 and the mean diameter varies between 5- 15 nm.
- 8. Classification of Lipoproteins Lipoproteins with high lipid content will have low density, larger size and so float on centrifugation. Those with high protein content sediment easily, have compact size and have a high density. 8
- 9. Classification of Lipoproteins 9 2) Based on electrophoretic mobilities Lipoproteins may be separated according to their electrophoretic properties into - α, pre β, β, and broad beta lipoproteins. The mobility of a lipoprotein is mainly dependent upon protein content. Those with higher protein content will move faster towards the anode and those with minimum protein content will have minimum mobility.
- 10. Classification of Lipoproteins Lipoproteins may be separated according to their electrophoretic properties into - α, pre β, β, and broad beta lipoproteins.
- 11. Classification of Lipoproteins 2) Based on electrophoretic mobilities (contd.) HDL are -α , VLDL pre- β, LDL-β , and IDL are broad beta lipoproteins. Free fatty acid and albumin complex although not a lipoprotein is an important lipid fraction in serum and is the fastest moving fraction. Chylomicrons remain at the origin since they have more lipid content. VLDLs with less protein content than LDL move faster than LDL, this is due to nature of apoprotein present.
- 12. Classification of Lipoproteins As the lipid content increases, density decreases and size increases, that is why Chylomicrons are least dense but biggest in size, while HDL are rich in proteins , hence most dense but smallest in size.
- 13. Classification of Lipoproteins 3) Based on nature of Apo- protein content One or more apolipoproteins (proteins or polypeptides) are present in each lipoprotein. The major apolipoproteins of HDL (α-lipoprotein) are designated A. The main apolipoprotein of LDL (β -lipoprotein) is apolipoprotein B (B-100), which is found also in VLDL. Chylomicons contain a shorten form of apo B (B- 48) that is synthesized in the intestine, while B-100 is synthesized in the liver. Apo E is found in VLDL, HDL, Chylomicons, and chylomicron remnants.
- 14. Functions of Apo proteins (1)They can form part of the structure of the lipoprotein, e.g. apo B, structural component of VLDL and Chylomicons (2)They are enzyme cofactors, e.g. C-II for lipoprotein lipase, A-I for lecithin: cholesterol acyl transferase (LCAT), or enzyme inhibitors, eg, apo A-II and apo C- III for lipoprotein lipase, apo C-I for cholesteryl ester transfer protein (3)They act as ligands for interaction with lipoprotein receptors in tissues, e.g. apo B-100 and apo E for the LDL receptor, apo A-I for the HDL receptor.
- 15. Lipoproteins Site Of Synthesis Destination Major Lipids Biochemical Functions Chylomicron s Intestine Liver Exogenous Triacylglycerol Deliver lipids of dietary origin to Liver and Adiposecytes VLDLs Liver Extra Hepatic Tissues Endogenous Triacylglycerol Deliver endogenously produced Lipids to Extrahepatocytes LDLs Intravascular by removal of triacylglycerol from VLDL Extra hepatic Tissues Cholesterol Deliver endogenously produced cholesterol to Extrahepatocytes HDLs Liver and intestine Liver and steroid- hormone- producing glands Phospholipid Cholesterol Remove and degrade Cholesterol.
- 16. Plasma Lipoproteins For Triacylglycerol Transport (TAG-rich): - Chylomicrons: TAG of dietary origin - VLDL:TAG of Endogenous (hepatic) synthesis For Cholesterol transport (cholesterol-rich): LDL: Mainly Free Cholesterol HDL: Mainly esterified Cholesterol
- 17. Metabolism of Chylomicrons Synthesis of Chylomicrons Chylomicrons are the transport form of dietary triglycerides from intestines to the adipose tissue for storage; and to muscle or heart for their energy needs. Chylomicrons are formed in the intestinal mucosal cells, and secreted into the lacteals of lymphatic system. They are rich in triglyceride If lipemic serum is kept overnight in the refrigerator, chylomicrons rise as a creamy layer to the top, leaving the subnatant clear When the chylomicrons are synthesised by the intestinal mucosa, they contain only apo-B-48 and apo-A but apo-C and apo-E are added from HDL in blood during transport
- 18. Chylomicron assembly Fatty acids, 2-MAG Fatty acids, 2-MAG ATP ADP Triacylglycerol Apolipoproteins Chylomicrons Chylomicrons lumen intestinal epithelium lymphatics Protein Triacylglycerol
- 20. Metabolism of Chylomicrons Main sites of metabolism of chylomicrons are adipose tissue and skeletal muscle. The half life of chylomicrons in blood is about 1 hour. The enzyme lipoprotein lipase (LpL) is located at the endothelial layer of capillaries of adipose tissue, muscles and heart; but not in liver. Apo C-II present in the chylomicrons activates the LpL The LpL hydrolyses triglycerides present in chylomicrons into fatty acids and glycerol. Muscle or adipose tissue cells take up the liberated fatty acids
- 21. Metabolism of Chylomicrons cont.. Following injection of heparin, the LpL is released from the tissues and lipemia is thus cleared. This is called post-heparin lipolytic activity. Lack of Apo C-II leads to decreased activity of LpL and consequent accumulation of chylomicrons and VLDL in blood Insulin increases LpL activity And Liver takes up Chylomicron remnants
- 23. Metabolism of VLDL Synthesis of VLDL There are striking similarities in the mechanisms of formation of chylomicrons by intestinal cells and of VLDL by hepatic parenchymal cells They are synthesized in the liver from glycerol and fatty acids and incorporated into VLDL along with hepatic cholesterol, apo-B-100, C-II and E. Apo-B-100 is the major lipoprotein present in VLDL VLDL carries triglycerides (endogenous triglycerides) from liver to peripheral tissues for energy needs. The half-life of VLDL in serum is only 1 to 3 hours.
- 24. VLDLAssembly TG/CE B48 cholesterol (exogenous) CE/TG B100 Dietary Carbohydrate glucose pyruvate Acetyl CoA mitochondria Acetyl CoA TG FFA FFA TG VLDL LIVER VLDL CMr Cholesterol (endogenous) E LDL receptor Plasma
- 25. Metabolism of VLDL Cont… When they reach the peripheral tissues, apo-C-II activates LpL which liberates fatty acids that are taken up by adipose tissue and muscle. The remnant is now designated as IDL intermediate density lipoprotein) and contains less of TAG and more of cholesterol The major fraction of IDL further loses triglyceride, so as to be converted to LDL This conversion of VLDL to IDL and then to LDL is referred to as lipoprotein cascade pathway A fraction of IDL is taken up by the hepatic receptors.
- 26. Metabolism of LDL LDL transports cholesterol from liver to peripheral tissues. The only apoprotein present in LDL is apo B100 Most of the LDL particles are derived from VLDL, but a small part is directly released from liver. The half-life of LDL in blood is about 2 days.
- 27. Metabolism of LDL Cont.. LDL is taken up by peripheral tissues by receptor mediated endocytosis The liver and many extra hepatic tissues express the IDL(apo B-100, E) receptor. This receptor is defective in familial hypercholesterolemia. Approximately 30% of LDL is degraded in extra- hepatic tissues and 70% in the liver. A positive correlation exists between the incidence of coronary atherosclerosis and the plasma concentration of LDL cholesterol.
- 28. LDL transports cholesterol from liver to the peripheral tissues. The cholesterol thus liberated in the cell has three major fates. i. It is used for the synthesis of other steroids like steroid hormones. ii. Cholesterol may be incorporated into the membranes. iii. Cholesterol may be esterified to a MUFA by acyl cholesterol acyl transferase (ACAT) for storage. iv. The cellular content of cholesterol regulates further endogenous synthesis of cholesterol by regulating HMG CoA reductase
- 29. LDL and Clinical Applications • LDL concentration in blood has positive correlation with incidence of cardiovascular diseases • A fraction of cholesterol is taken up by macrophages, this is not a regulated pathway. • Increased levels of LDL or modification of LDL by glycation (as seen in diabetes mellitus) or oxidation increases the fraction of cholesterol taken up by macrophages. • LDL infiltrates through arterial walls, and is taken up by macrophages or scavenger cells. This is the starting event of atherosclerosis leading to myocardial infarction
- 30. LDL and Clinical Applications Cont.. When these cells become engorged (swell) with cholesterol, foam cells are formed, that get deposited in the sub-endothelial space triggering formation of athero-matous plaque Pro-coagulant changes are induced in the endothelium resulting in increased chances of thrombosis and coronary artery disease Since LDL-cholesterol is thus deposited in tissues, so known as “bad cholesterol”
- 31. Lipoprotein (a) Lipoprotein (a) or Lp(a) should not be confused with apo-A. Lp(a) is very strongly associated with myocardial infarction and is sometimes called the “little rascal”. Lp(a), when present, is attached to apo-B-100 by a disulfide bond. In 40% population, there is no detectable level of Lp(a) in serum. In 20% of population, the Lp(a) concentration in blood is more than 30 mg/dl; and these persons are susceptible for heart attack at a younger age. Apo-A is a constituent of HDL. This "A" is always written in capital letters. It is seen in all persons. It is anti- atherogenic.
- 32. The biochemical analysis of plasma from a patient with pancreatitis showed hypertriglyceridemia with increased VLDL and chylomicrons. To further investigate, the patient was administered heparin intravenously and blood samples were collected to analyze the lipolytic activity in plasma. The test showed low LPL activity in post heparinized blood samples. Identify the probable cause of reaction after an intravenous heparin injection increased VLDL and Chylomicrons A) Deficiency of Apo B b) Deficiency of Lipoprotein Lipase c) Deficiency of LDL receptor d) Deficiency of Apo A-I Deficiency of Lipoprotein Lipase
- 33. Familial Hypercholesterolemia is an autosomal dominant genetic disorder caused by a mutation of the gene that encodes for: a) Apolipoprotein E b) Apolipoprotein B c) LDL receptor d) VLDL receptor LDL receptor
- 34. The lipoprotein lipase is present in the endothelial surfaces of adipose tissues in the heart and it is required for hydrolysis and release of triglycerides from chylomicrons. Which of the apolipoprotein that is present in chylomicron serves as the activator of an enzyme lipoprotein lipase? a) Apo B100 b) Apo B48 c) Apo CII d) ApoE Apo CII
- 36. Metabolism of HDL Synthesis of HDL High density lipoproteins transport cholesterol from peripheral tissues to the liver. HDL is synthesized and secreted from both liver and intestine . The major apoproteins in HDL are Apo-A1, with some Apo-A2, Apo-C and Apo-E. However, apo C and apo E are synthesized in the liver and transferred from liver HDL to intestinal HDL when the latter enters the plasma.
- 37. Metabolism of HDL cont.. A major function of HDL is to act as a repository for the apo C and apo E required in the metabolism of chylomicrons and VLDL. The free cholesterol derived from peripheral tissue cells are taken up by the HDL. The apo-A-l of HDL activates LCAT (lecithin cholesterol acyl transferase) present in the plasma. • The LCAT then binds to the HDL which is components of phospholipid bilayer of the HDL disk.
- 38. Metabolism of HDL cont.. 38 LCAT and the LCAT activator apo A-I—bind to the discoidal particles, and the surface phospholipid and free cholesterol are converted into cholesteryl esters and lysolecithin . T h e nonpolar cholesteryl esters move into t h e hydrophobic interior of the bilayer, whereas lysolecithin is transferred to plasma albumin. Thus, a nonpolar core is generated, forming a spherical, pseudomicellar HDL covered by a surface film of polar lipids and apolipoproteins. This aids the removal of excess unesterified cholesterol from lipoproteins and tissues .
- 39. Reverse cholesterol transport Reverse cholesterol transport is a mechanism by which the body removes excess cholesterol from peripheral tissues and delivers them to the liver, where it will be redistributed to other tissues or removed from the body by the gallbladder. 39
- 40. Metabolism of HDL T h e class B scavenger receptor B1 (SR-B1) has been identified as an HDL receptor with a dual role in HDL metabolism. In the liver and in steroidogenic tissues, it binds H D L via apo A-I, and cholesteryl ester is selectively delivered to the cells, although the particle itself, including apo A-I, is not taken up. I n the tissues, on the other hand, SR-B1 mediates t h e acceptance of cholesterol from the cells by HDL, which then transports it to the liver for excretion via the bile (either as cholesterol or after conversion to bile acids) in the process known as reverse transport 33
- 41. HDL- cycle HDL3, generated from discoidal HDL by the action of LCAT, accepts cholesterol from the tissues via the SR- B1 and the cholesterol is then esterified by LCAT, increasing the size of the particles to form the less dense HDL2. HDL3 is then reformed, either after selective delivery of cholesteryl ester to the liver via the SR-B1 or by hydrolysis of HDL2 phospholipid and triacylglycerol by hepatic lipase. This interchange of HDL2 and HDL3 is called the HDL cycle. Free apo A-I is released by these processes andforms pre -HDL after associating with a minimum amount of phospholipid and cholesterol 34
- 42. Functions of HDL Scavenging action- HDL scavenges extra cholesterol from peripheral tissues by reverse cholesterol transport HDL, with the help of apo E competes with LDL for binding sites on the membranes and prevents internalization of LDL cholesterol in the smooth cells of the arterial walls H D L contributes its apo C and E to nascent VLDL a n d chylomicrons for receptor mediated endocytosis H D L stimulated prostacyclin synthesis by the endothelial cells, which prevent thrombus formation H D L also helps in the removal of macrophages. 36
- 43. Summary of formation and fate Chylomicrons is a transporter of dietary lipids whereas VLDL is a transporter of endogenous lipids(mainly TGs). LDL transports cholesterol to peripheral cells while HDL transports cholesterol from peripheral cells back to liver 37
- 44. Clinical Significance of lipoprotein metabolism 44 Fatty Liver Is an abnormal accumulation of certain fats (triglycerides) inside liver cells. Hepatic triacylglycerol synthesis provides the immediate stimulus for the formation and secretion of VLDL. Impaired VLDL formation or secretion leads to nonmobilization of lipid components from the liver, results in fatty liver.
- 45. Fatty Liver (contd.) Fatty livers fall into two main categories- A)More synthesis of Triglycerides High carbohydratediet High fat feeding Starvation Diabetes mellitus High carbohydrate diet stimulates de novo fatty acid synthesis by providing excess of Acetyl CoA and high fat feeding provides more flux of fatty acids from the diet that can be esterifies to provide excess Triglyceride. 40
- 46. Fatty Liver
- 47. Fatty Liver (contd.) 47 B) Defective VLDL synthesis -The second type of fatty liver is usually due to a metabolic block in the production of plasma lipoproteins, thus allowing triacylglycerol to accumulate. It may be due to – (1)A block in apolipoproteins synthesis a) Protein energy Malnutrition b) Impaired absorption c)Presence of inhibitors of endogenous protein synthesis e.g.- Carbon tetra chloride, Puromycin, Ethionine , Heavy metals etc. d)Hypobetalipoproteinemia- Defective apo B gene can cause impaired synthesis of apo B protein.
- 48. Fatty Liver (contd.) 48 (2) A failure in provision of phospholipids that are found in lipoproteins a)A deficiency of choline, a lipotropic factor can cause impaired formation of phosphatidyl choline (Lecithin),a glycerophospholipid. b)Methionine deficiency can also cause impaired choline synthesis c)Deficiency of essential fatty acids can also cause impaired PL synthesis
- 49. Fatty Liver (contd.) • (3) Impaired Glycosylation- Orotic acid also causes fatty liver; it interferes with glycosylation of the lipoprotein, thus inhibiting release, and may also impair the recruitment of triacylglycerol to the particles. In conditions of orotic aciduria(disorder of pyrimidine nucleotide biosynthesis), fatty liver can be observed. • 4) Impaired secretion of VLDL- oxidative stress is a common cause for membrane disruption of lipoproteins. 49
- 50. Fatty Liver (contd.) 50 2) Alcoholic fatty liver Alcoholism leads to fat accumulation in the liver, hyperlipidemia, and ultimately cirrhosis. The fatty liver is caused by a combination of impaired fatty acid oxidation and increased lipogenesis, which is thought to be due to changes in the [NADH]/ [NAD+] redox potential in the liver, and also to interference with the action of transcription factors regulating the expression of the enzymes involved in the pathways.
- 51. Fatty Liver and Lipotropic agents 51 Lipotropic agents- Agents such as- •Choline •Inositol •Methionine and other essential amino acids, • Essential fatty acids, •Anti oxidant vitamins, •Vitamin B12, folic acid and •Synthetic antioxidants which have the apparent effect of removal of fats from the liver cells, and thus prevent the formation of fatty liver are called lipotropic agents.
- 52. Primary Disorders of Plasma Lipoproteins (Dyslipoproteinemias) • Inherited defects in lipoprotein metabolism lead to the primary condition of either hypo- or hyperlipoproteinemia . • In addition, diseases such as diabetes mellitus, hypothyroidism, nephrotic syndrome, and atherosclerosis are associated with secondary abnormal lipoprotein patterns that are very similar to one or another of the primary inherited conditions. • All of the primary conditions are due to a defect at a stage in lipoprotein formation, transport, or degradation. 52
- 53. Primary Disorders of Plasma Lipoproteins (Dyslipoproteinemias) 53 Name Defect Characteristics Hypolipoproteinemias Abetalipoproteinemia Rare; blood acylglycerols low; intestine and liver accumulateacylglycerols. Intestinal malabsorption. No chylomicrons, VLDL, or LDL are formed because of defect in the loading of apo B with lipid. All have low or near absence of HDL. Hypertriacylglycerolemia due to absence of apo C- II, Low LDL levels. Atherosclerosis in the elderly. Familial alpha- lipoprotein deficiency Tangier disease Fish-eye disease Apo-A-I deficiencies
- 54. Primary Disorders of Plasma Lipoproteins (Dyslipoproteinemias) 54 Defect Characteristics Name Hyperlipoproteinemia Familial lipoprotein lipase deficiency (type I) Familial hypercholesterolemia (type II a) Hypertriacylglycerolemia due to deficiency of LPL, abnormal LPL, or apo C- II deficiency causing inactive LPL. Defective LDL receptors or mutation in ligand region of apo B-100. Slow clearance of chylomicrons and VLDL. Low levels of LDL and HDL. No increased risk of coronary disease. Elevated LDL levels and hypercholesterolemia, resulting in atherosclerosis and coronary disease.
- 55. Primary Disorders of Plasma Lipoproteins (Dyslipoproteinemias)- contd. Name Defect Characteristics Deficiency in remnant clearance by the liver is due to abnormality in apo E. Familial type III hyperlipoproteinemia (broad beta disease, remnant removal disease, familial dysbetalipoproteinemia) Familial Hypertriacylglycerolemia (type IV) Overproduction of VLDL often associated with glucose intolerance and hyperinsulinemia. Hepatic lipase deficiency Deficiency of the enzyme leads to accumulation of large triacylglycerol-rich Increase in chylomicron and VLDL remnants , Causes hypercholesterolemia, xanthomas, and atherosclerosis. High cholesterol, VLDL, Subnormal LDL and HDL. Associated with Alcoholism, diabetes mellitus and obesity. Patients have xanthomas and coronary heart disease. 50
- 56. 1. The class of lipoproteins that is protective against atherosclerosis is … a. Low-density of lipoproteins b. Very low-density lipoproteins c. High-density lipoproteins d. Chylomicrons High-density lipoproteins
- 57. 2. The highest phospholipids content is found in a. Chylomicrons b. VLDL c. LDL d. HDL HDL
- 58. 3. Activated lecithin cholesterol acyl transferase is essential for the conversion of ... a. VLDL remnants into LDL b. Nascent HDL into HDL c. HDL2 into HDL3 d. HDL3 into HDL2 HDL3 into HDL2
Editor's Notes
- c
- d
- d