This document discusses lipid and lipoprotein metabolism. Key points include:
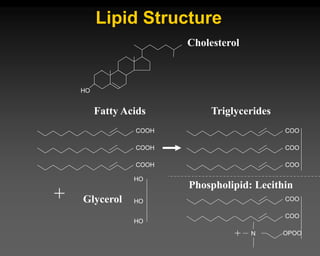
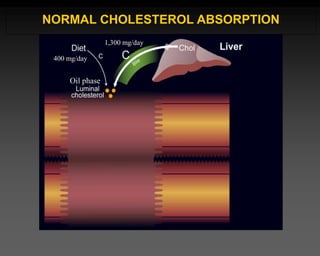
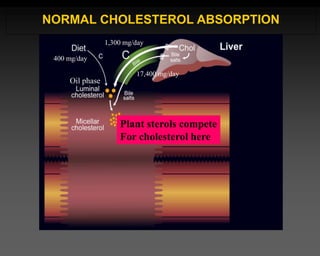
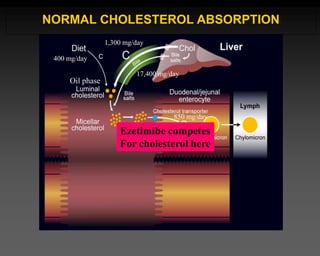
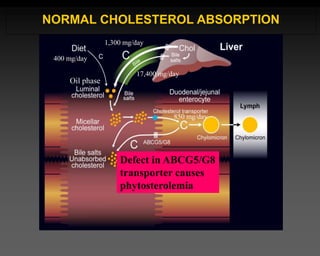
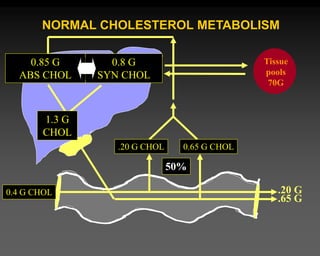
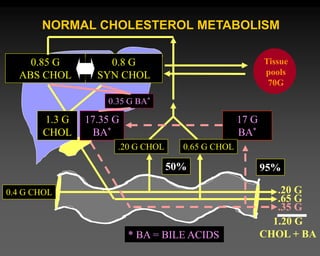
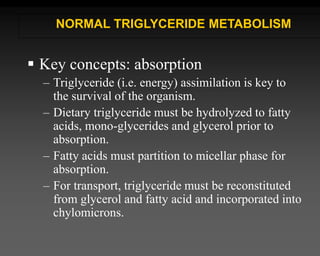
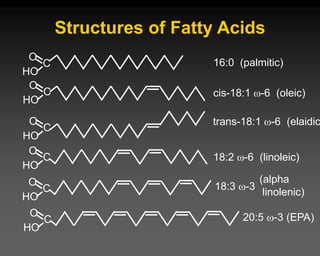
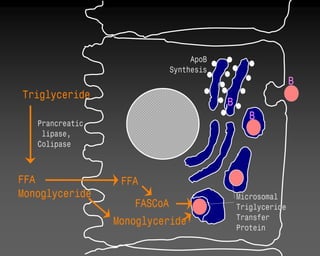
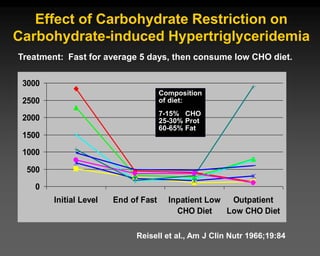
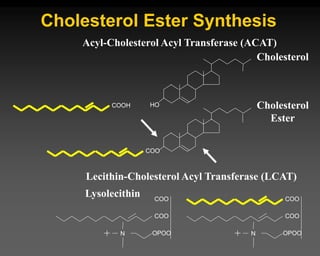
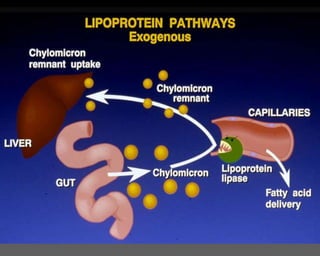
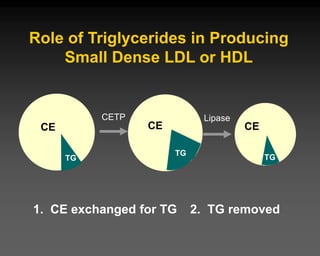
1) Cholesterol is synthesized in tissues and absorbed from the diet, while triglycerides are absorbed after dietary fat is broken down.
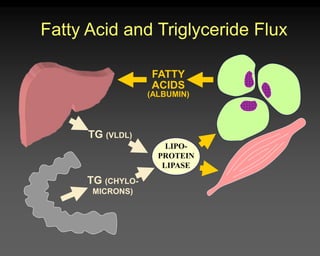
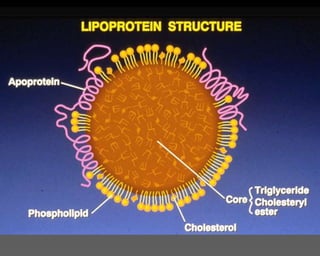
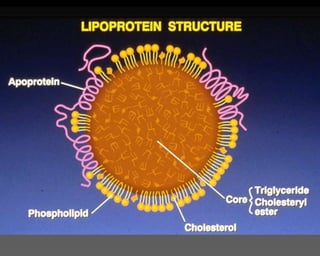
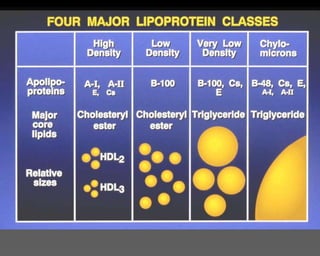
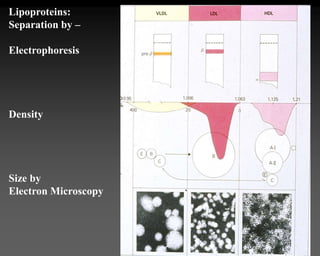
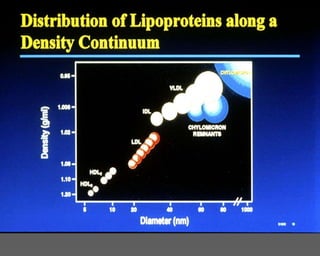
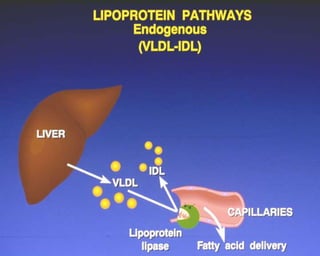
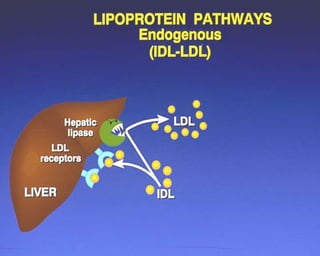
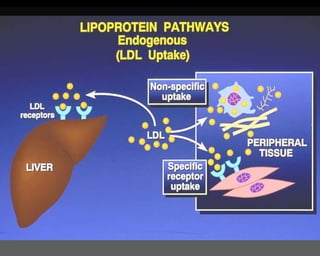
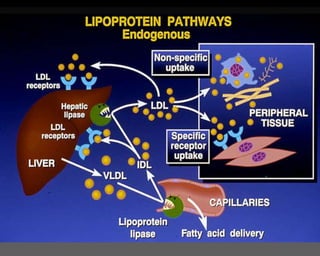
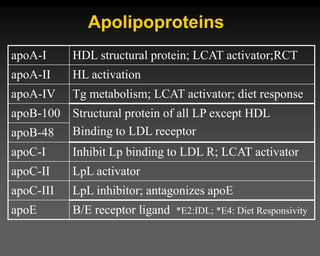
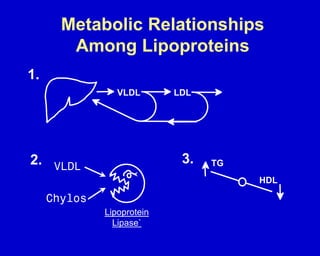
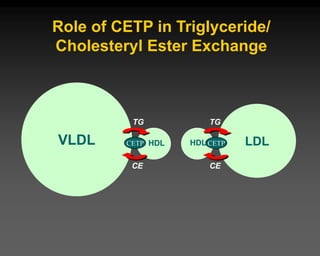
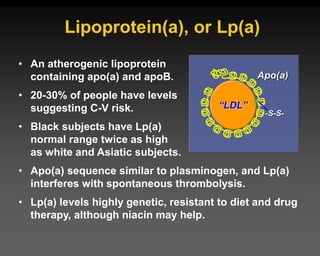
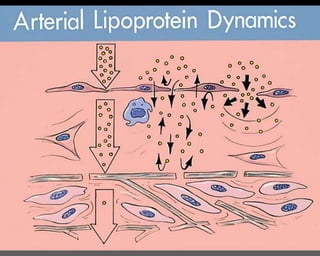
2) Lipoproteins like LDL and HDL transport lipids in the blood and are composed of a lipid core surrounded by proteins and phospholipids.
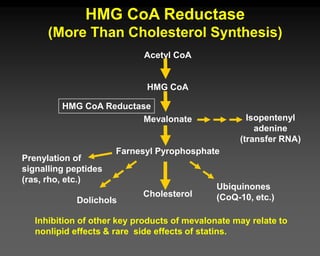
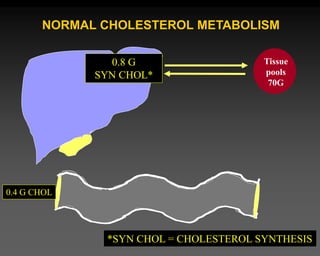
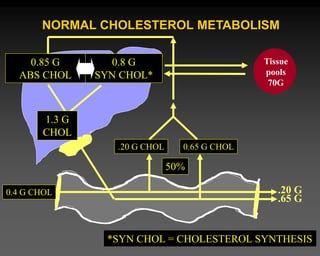
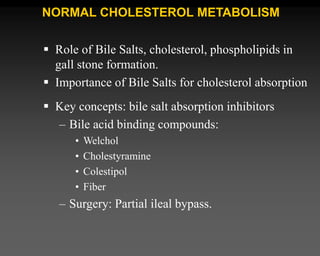
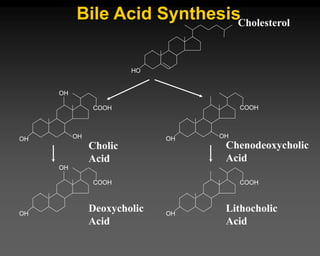
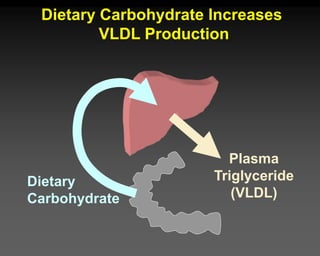
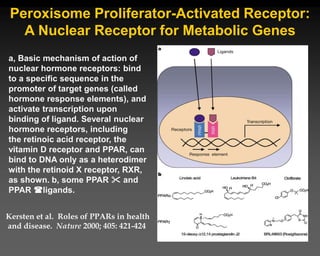
3) The liver plays a central role in lipid homeostasis, regulating cholesterol synthesis and bile acid production.
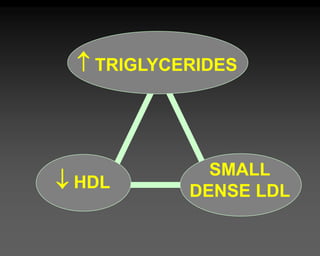
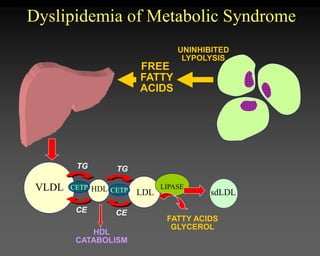
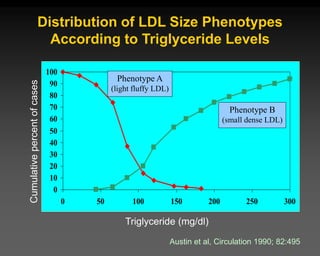
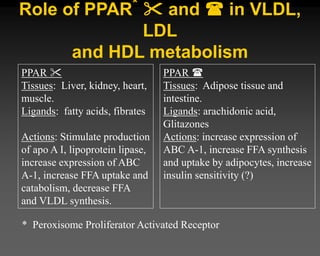
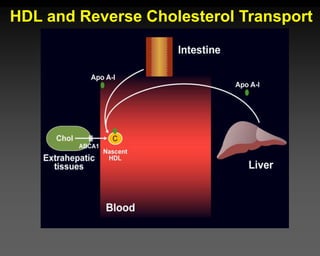
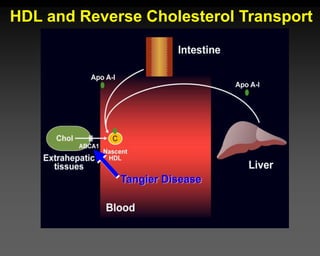
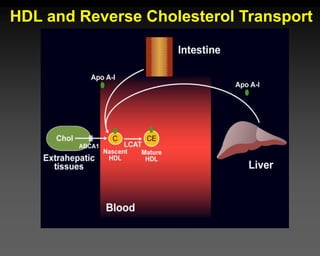
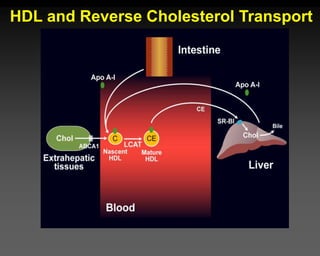
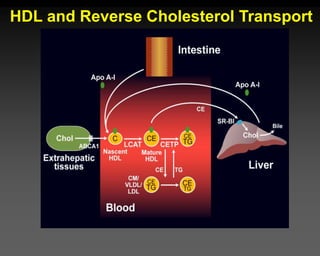
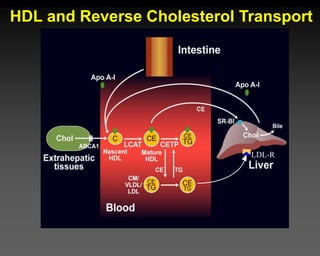
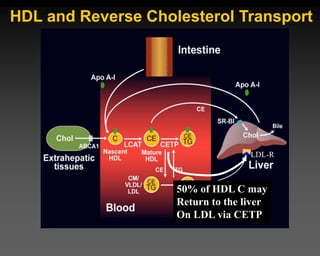
4) Derangements in lipid metabolism can occur in conditions like metabolic syndrome and increase disease risk. Reverse cholesterol transport via HDL is an important protective process.















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



