Lipid-derived autacoids are a group of endogenous bioactive lipid molecules derived primarily from arachidonic acid and other polyunsaturated fatty acids. These molecules act locally and transiently to modulate inflammation, pain, fever, platelet aggregation, and other physiological processes. The main classes include prostaglandins, thromboxanes, leukotrienes, and platelet-activating factor (PAF).
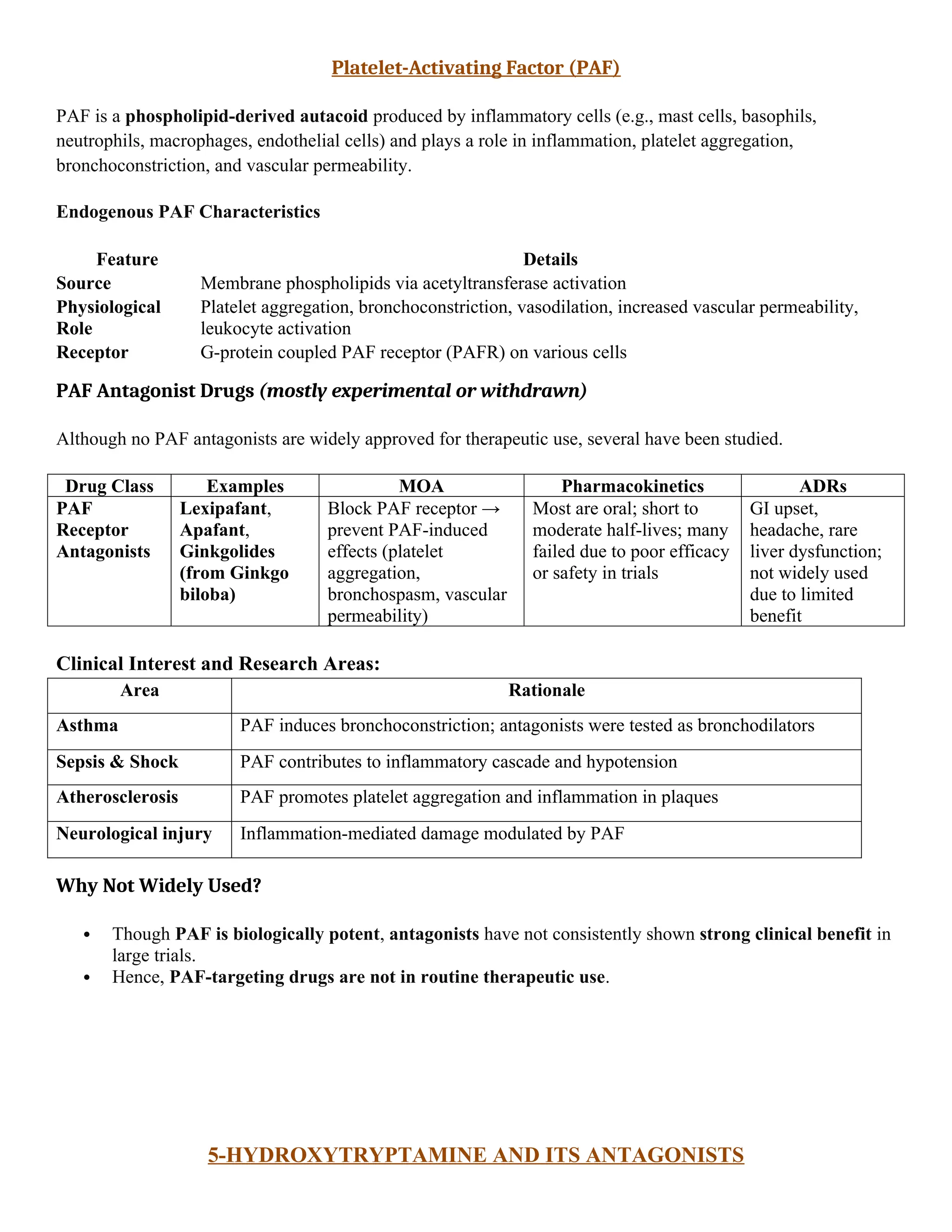
PAF is a phospholipid-derived autacoid produced by inflammatory cells (e.g., mast cells, basophils, neutrophils, macrophages, endothelial cells) and plays a role in inflammation, platelet aggregation, bronchoconstriction, and vascular permeability.
5-Hydroxytryptamine (5-HT), also known as serotonin, is a biogenic amine that acts as a neurotransmitter and autacoid. It has multiple receptor subtypes (5-HT1 to 5-HT7), and both agonists and antagonists of these receptors are used as therapeutic drugs in various conditions.
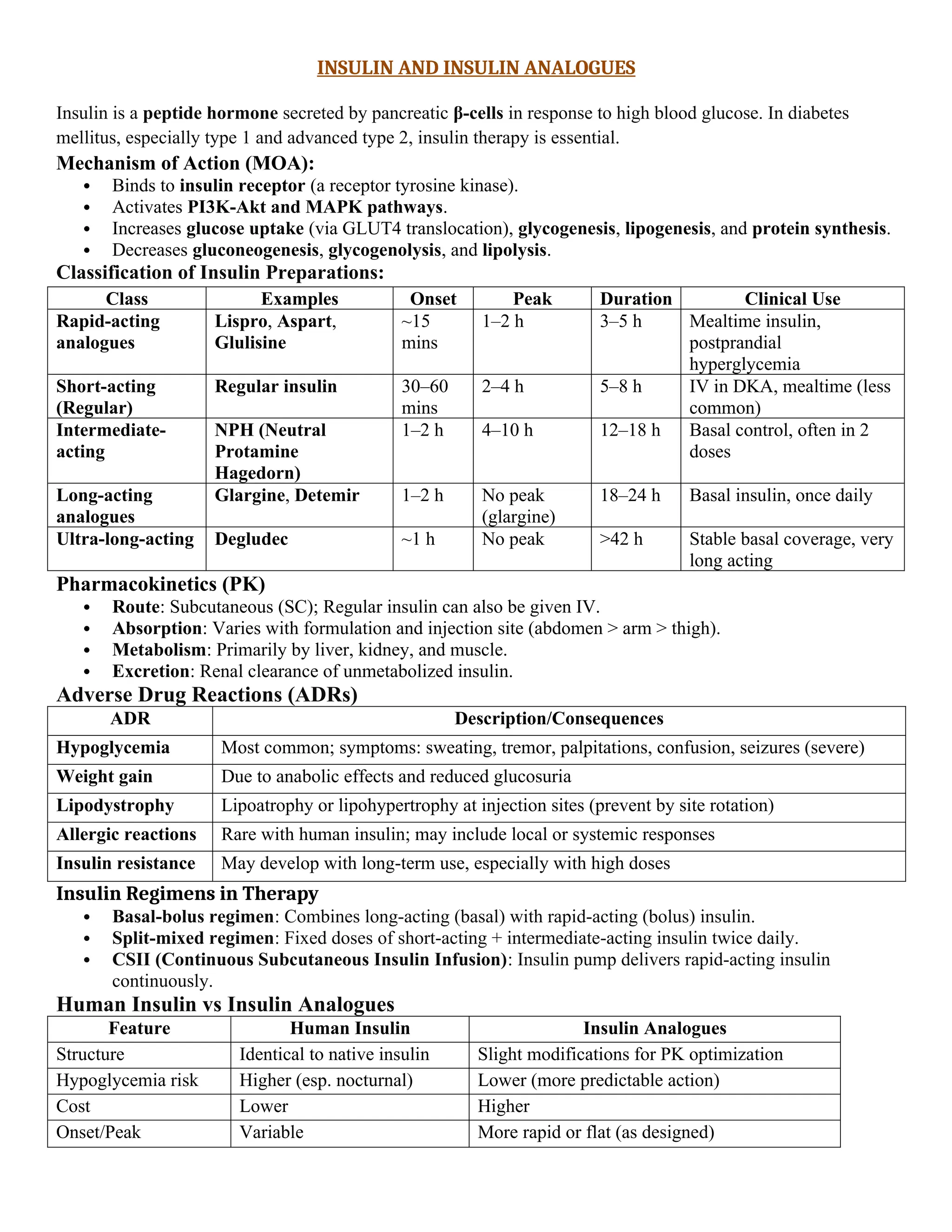
Insulin is a peptide hormone secreted by pancreatic β-cells in response to high blood glucose. In diabetes mellitus, especially type 1 and advanced type 2, insulin therapy is essential.
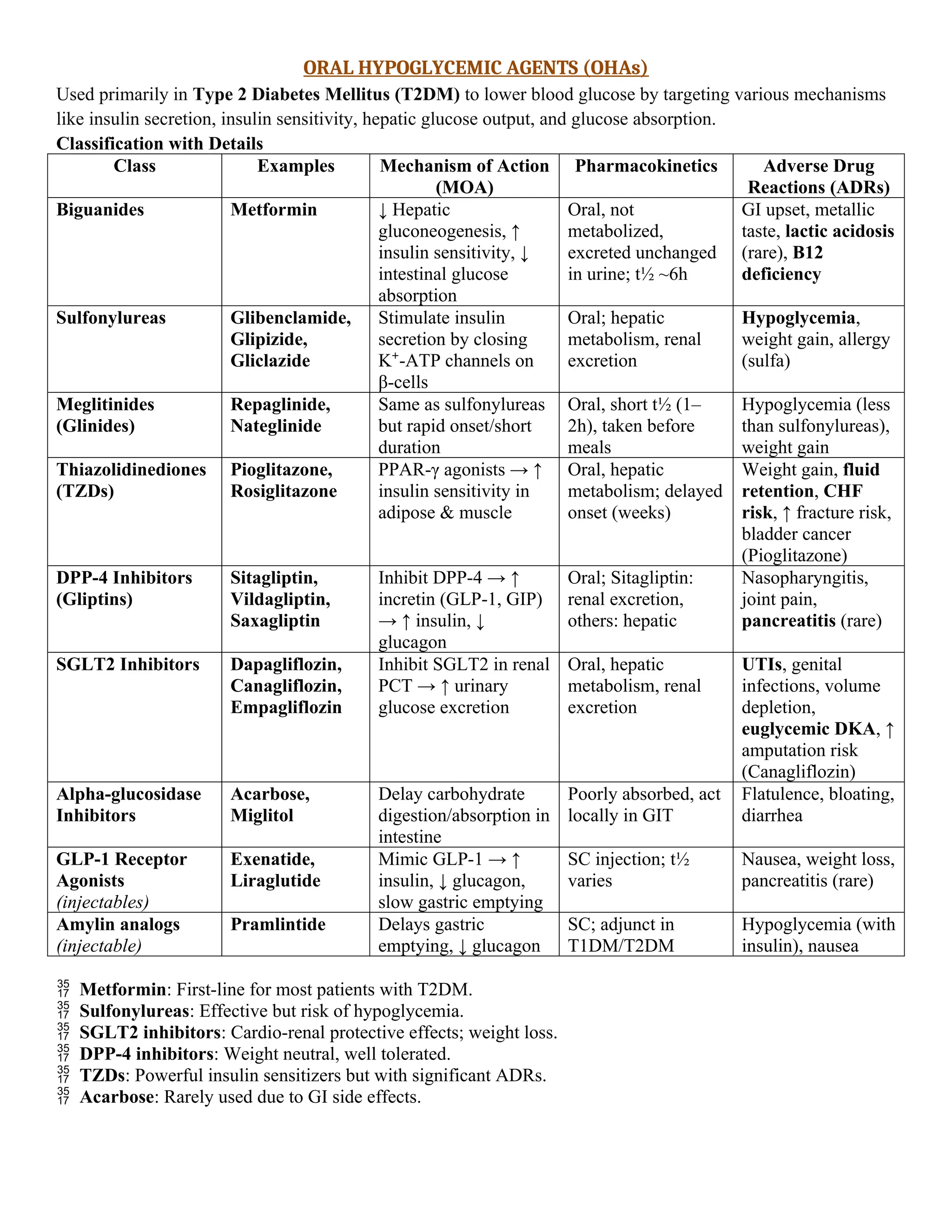
Oral Hypoglycemic Agents (OHAs)
Used primarily in Type 2 Diabetes Mellitus (T2DM) to lower blood glucose by targeting various mechanisms like insulin secretion, insulin sensitivity, hepatic glucose output, and glucose absorption.
Analgesics and anti inflammatory agents.