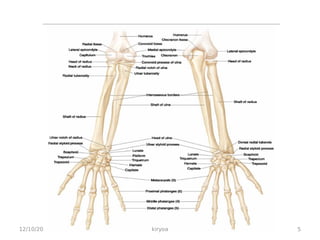
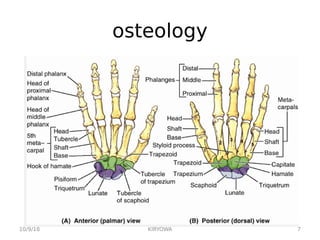
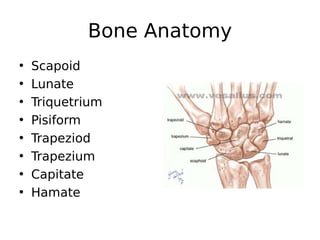
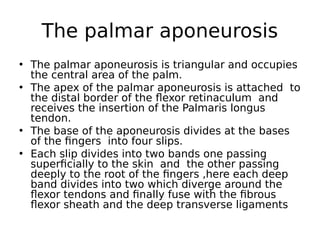
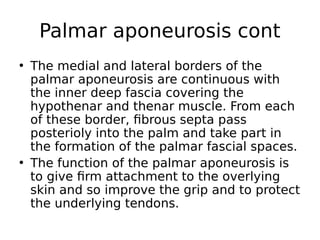
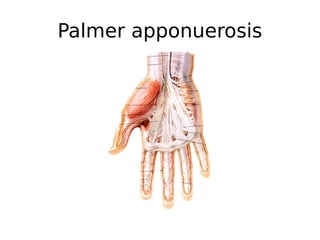
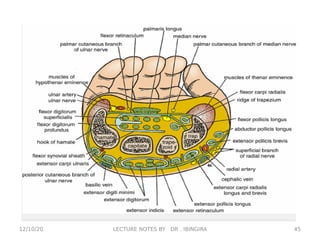
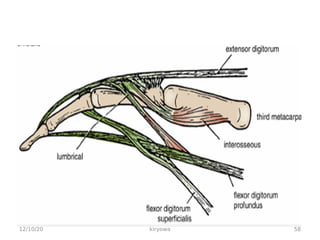
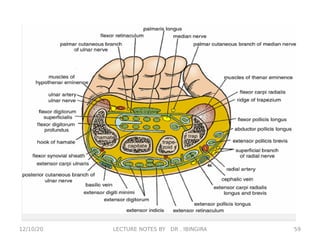
The document provides an overview of the anatomy of the hand and wrist region. It begins with definitions of key terms and descriptions of the bones that make up the hand, including 8 carpal bones, 5 metacarpal bones, and 14 phalanges. It then discusses the dorsal and palmar surfaces in more detail, describing structures like the palmar aponeurosis and flexor retinaculum. The document also provides brief summaries of the embryological development of the hand and some common congenital anomalies that can occur.


![The spaces of the hand
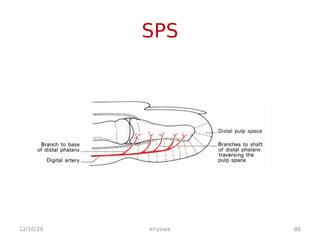
• superficial pulp spaces of the
superficial pulp spaces of the
fingers
fingers
• synovial tendon sheaths of the
synovial tendon sheaths of the
2
2nd
nd
, 3
, 3rd
rd
, 4
, 4th
th
fingers
fingers
• the ulna bursa
the ulna bursa
• the radial bursa[ FPL]
the radial bursa[ FPL]
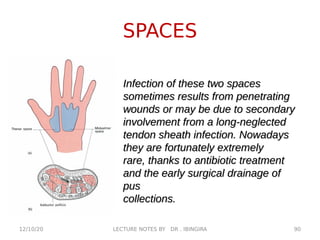
• the mid palmar space
the mid palmar space
• the thenar space
the thenar space
12/10/20 87
kiryowa](https://image.slidesharecdn.com/lecture6bthehanddr-230813200631-f484d231/85/lecture-6b-THE-HAND-Dr-kiryowa-1-pdf-87-320.jpg)
![BURSAE
The synovial
The synovial
sheaths of the flexor
sheaths of the flexor
tendons of the hand—the
tendons of the hand—the
Radial[FPL] and ulnar
Radial[FPL] and ulnar
bursae[ little finger.
bursae[ little finger.
track proximally deep to
track proximally deep to
the flexor retinaculum
the flexor retinaculum
and provide a potential
and provide a potential
pathway of infection into
pathway of infection into
the forearm. In many
the forearm. In many
cases these bursae
cases these bursae
communicate.
communicate.
12/10/20 89
LECTURE NOTES BY DR . IBINGIRA](https://image.slidesharecdn.com/lecture6bthehanddr-230813200631-f484d231/85/lecture-6b-THE-HAND-Dr-kiryowa-1-pdf-89-320.jpg)
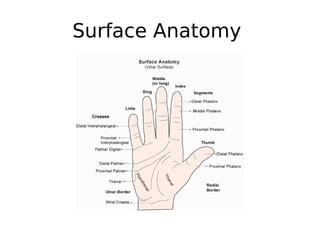
![MORE
• Dermatoglyphics e.g simian crease.
Dermatoglyphics e.g simian crease.
wrist creases[proximal, middle, distal],
wrist creases[proximal, middle, distal],
palmar creases[radial longitudinal,
palmar creases[radial longitudinal,
proximal transverse, distal transverse,
proximal transverse, distal transverse,
digital creases,
digital creases,
• Thumb has 2 creases
Thumb has 2 creases
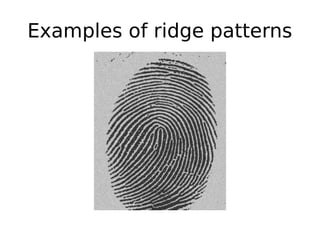
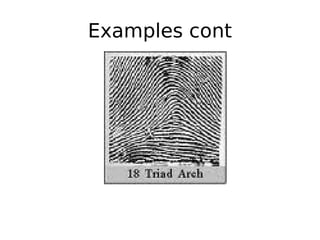
• Skin ridges- unique pattern, hence
Skin ridges- unique pattern, hence
finger prints.
finger prints.
• Reduce slippage when grasping.
Reduce slippage when grasping.
12/10/20 96
kiryowa](https://image.slidesharecdn.com/lecture6bthehanddr-230813200631-f484d231/85/lecture-6b-THE-HAND-Dr-kiryowa-1-pdf-96-320.jpg)