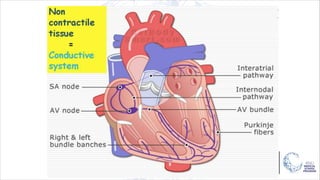
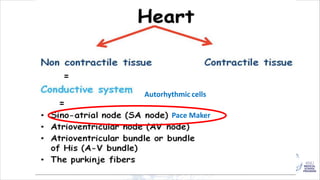
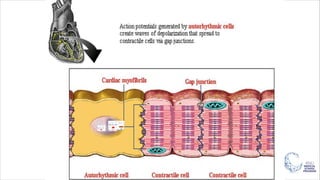
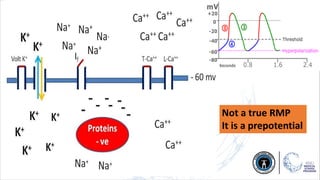
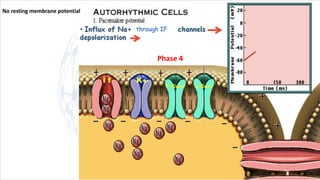
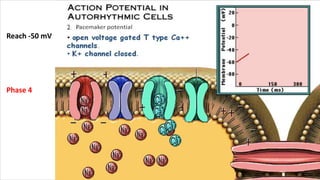
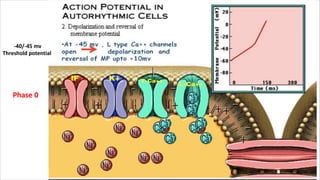
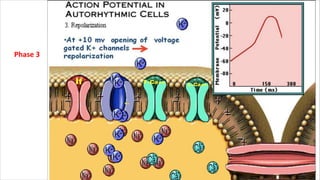
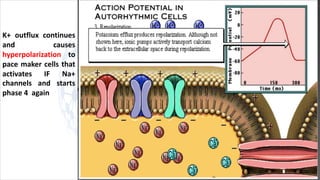
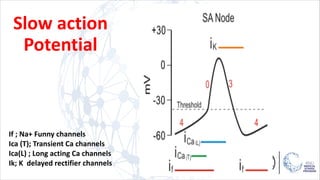
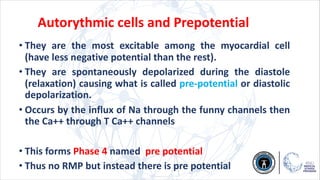
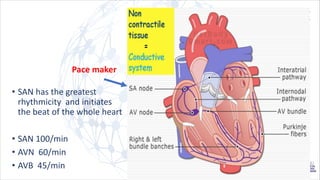
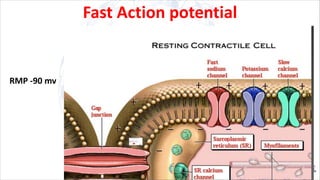
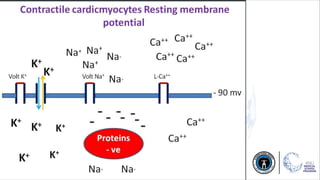
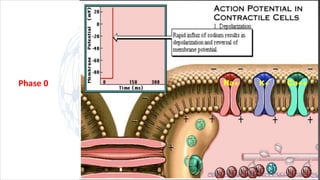
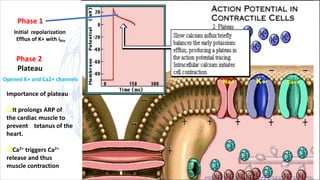
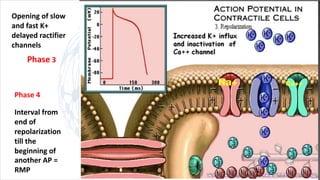
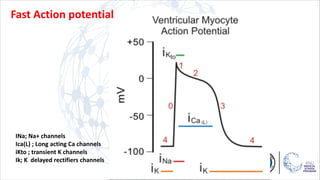
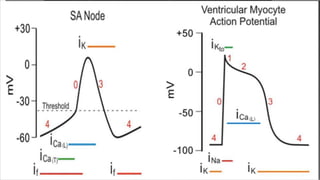
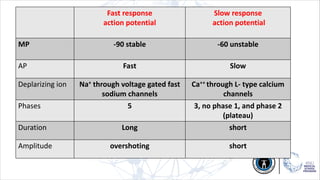
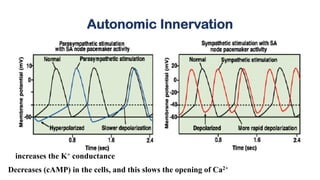
This document summarizes cardiac automaticity and the types of cardiac action potentials. It describes that the sinoatrial node contains pacemaker cells that spontaneously depolarize through sodium and calcium influx, generating a prepotential. This prepotential triggers the fast response action potential throughout the heart. The fast response action potential involves sodium influx in phase 0, followed by potassium efflux in phase 3, causing repolarization.