Laryngomalacia
•LM is acongenital softening of the
tissue sof the larynx and the
commonest cause of stridor in infants
3.
How would youapproach ? : History
• Histrory on Stridor : nature , factors aggravating, relieving
• Feeding : ? BM / FM / Volume vs Frequency/ Regurgitation
• Dusky spells : ?Cyanosis: peripheral/ central / duration/ sleep
• Birth Hx : Term / Weight / Apgar Score/ mode of delivery
• Perinatal Hx – TORCHES
• Other medical condition(s)
4.
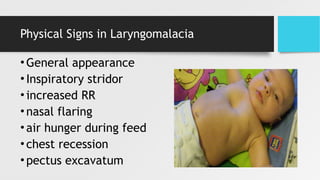
Laryngomalacia: History
• InspiratoryStridor
• may sound like nasal congestion, with which they are initially confused.
• No nasal secretions are present.
• Worsened in : supine, crying or agitation, URTI episodes , during and after feeding.
• In mild cases crying may improve symptoms
• The baby's cry is usually normal
• Usually, no feeding intolerance is noted
• The infant is usually happy and thriving (30% feeding problem with poor wt gain)
Flexible Nasolaryngoscopy
• Sufficein most cases
• Supraglottic collapse can be easily elicited
• Child can be followed up in 4 weeks
• Mostly isolated finding in otherwise healthy infant
15 – 20 % may have other co-existing lesions :
subglottic stenoses or laryngomalacia
9.
Indications for MLBin Laryngomalacia
1. Symptoms that do not correlate with degree of
laryngomalacia noted on FNL
2. Evaluate for co-existing airway lesions (12- 27%)
3. Evaluate for surgical intervention
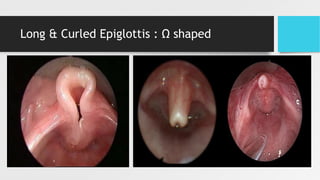
Layngomalacia : Holinger’sClassification
• Type 1: collapse of AE folds
• Type 2: tubular epiglottis with inward collapse
• Type 3: anteromedial collapse of the arytenoids, corniculates & cuneiform
• Type 4: posterior collapse of the epiglottis
• Type 5: shortened AE folds
Aspiration in Laryngomalacia
•25-72% of patients with severe laryngomalacia also have
aspiration
• Clinical swallow exam
• Video fluoroscopic swallow study (VFSS)
• Fiberoptic endoscopic evaluation of swallowing (FEES)
• Symptoms of aspiration:
• Coughing and choking with feeds
• Cyanosis, apnoeic episodes, respiratory distress around meal times
16.
Laryngomalacia : Management
•90% of children sx resolved by 2 yo
• Flexible scope in clinic is adequate
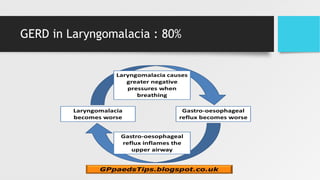
• BD PPI & reflux precaution (80% have GERD)
• DL & bronchoscopy (for severe cases): spontaneous
breathing to allow a complete, dynamic assessment of
airway
17.
Laryngomalacia : Indicationsfor surgery
1. failure to thrive (<5%)
2. cyanotic episodes and persistent stridor with accessory
muscle usage
3. significantly elevated carbon dioxide or hypoxemia
4. severe obstructive sleep apnea
5. pulmonary hypertension
6. cor pulmonale
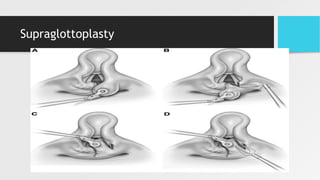
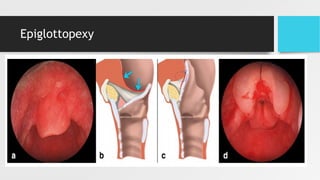
Supraglottoplasty : Benefits
•Well tolerated procedure
• High success rate
• 69-94% with resolution of airway and feeding symptoms
• Improvement of reflux, aspiration and sleep apnea
• Low failure rate
• 1-3% need tracheotomy
• Typically patients with associated neurologic disorder or syndrome
• Discoordinate pharyngolaryngomalacia
Further Work up
1.Assessment of swallowing
• Barium swallow/ MLB/ FEES
• Assessment for reflux and
aspiration
2.. Airway Fluoroscopy
• Dynamic study
• Supplement to endoscopy to
evaluate subglottis and trachea
3. CXR / Neck XR
• Croup
• Foreign body
• Pneumonia
4. PSG
• To evaluate apnoea
• Central obstructive
5. Echocardiogram
• Check for cardiac origin of cyanosis
• Preoperative clearance
• Effects of OSA
25.
Take home messages
•Congenital inspiratory stridor – most due to supraglottic collapse
• 80-90% resolve by 1-2 years of age with
conservative mx
• Strong association with GERD
• Aspiration and sleep apnoea are common cx
• Silent chest and diminished RR Raise red flag
• More severe symptoms warrant surgical intervention
Editor's Notes
#14 The relationship is proven with operative specimen histological studies
#15 Altered anatomy and neuromuscular reflexes :dysfunction of suck-swallow-breathe sequence
Disruption of Laryngeal Adductor Reflex (LAR) : laryngeal penetration
Failure of Closure of vocal cords and cessation of breathing as food passes into pharynx
Rapid feeding aspiration: Increased metabolic demands, weight loss, hunger
#22 Richter, Thompson et al: 31/36 pts had resolution from pre-op aspiration
Supraglottoplasty doesn’t cause post op aspiration ; 0/14