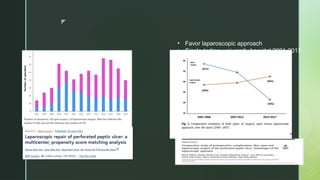
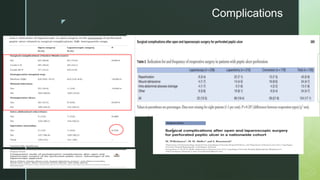
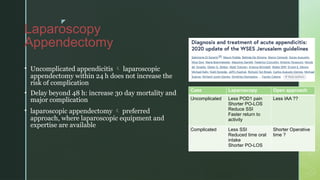
The management of perforated peptic ulcers emphasizes timely surgical intervention, with laparoscopic approaches recommended for stable patients and specific criteria for surgical repair based on size. Evidence from five university hospitals in South Korea suggests that laparoscopic methods lead to fewer complications and quicker recovery, particularly in uncomplicated cases. Overall, a focus on skilled surgical techniques and enhanced recovery protocols is vital for improving patient outcomes.