INTRODUCTION
Lactic acidis the normal endpoint of the anaerobic
breakdown of glucose in the tissues
Normal plasma lactate: 0.5 to 1.5 meq/L
3.
DEFINITION
Lactic acidosisis a pathological state diagnosed when the
serum concentration of lactate or lactic acid is
persistently 5mmol/l or greater
There is significant acidemia and serum pH< 7.35
4.
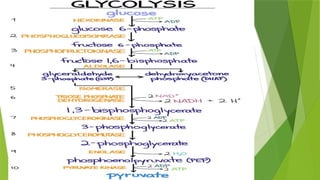
FORMATION OF LACTICACID
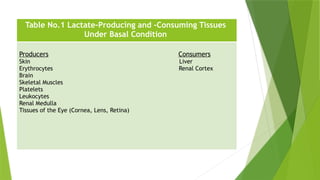
RBCs, brain and skin are major sources of lactic acid
During exercise skeletal muscles release significant
amount of lactic acid
Liver and kidneys utilize lactic acid for biosynthesis of
glucose
It is catalyzed by the enzyme lactate dehydrogenase
5.
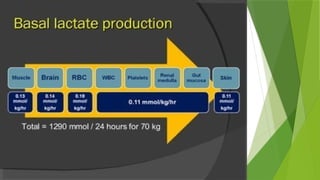
The bodytissues produces 1500 mmoles of lactate each
day
The lactate enters blood stream and metabolized meanly
by liver (60% in Cori Cycle) and kidneys (30%) to glucose
All tissues can produce lactate under anaerobic conditions
Skeletal muscles produce high amounts of lactate during
vigorous exercise
Oxygen may not reach the muscle fast enough to keep up
with the workout
LACTATE METABOLISM IN TISSUE
8.
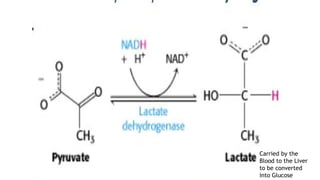
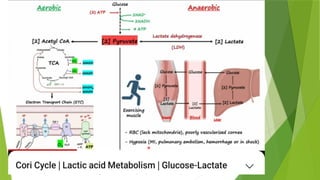
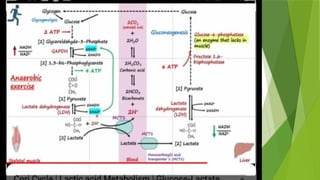
PYRUVATE TO LACTATE
The reduction of pyruvate by NADH+ catalyzed by to form lactate by lactate
dehydrogenase on anaerobic glycolysis to generate ATP
The reaction takes place in the cells when the amount of oxygen is less, as in
muscle during intense activity
Pyruvate lactate regenerates NAD+ which prevents glycolysis from cease to
function
Lactate cannot be used to generate energy
Lactate must be removed from the muscles to prevent lactic acidosis
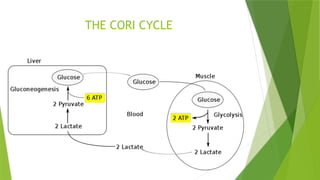
CORI CYCLE
Itis named after Carl Cori and Gerty Cori in 1929
It is also known as lactic acid cycle or glucose lactate or lactic acid
fermentation
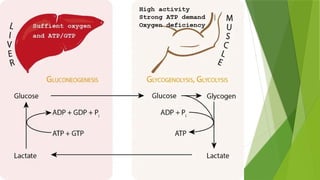
It involves the synthesis of glucose through gluconeogenesis from lactate
synthesized in the skeletal muscle
It occurs when the muscles need energy or during hypoxia
-Intense exercise
-Sprinting
PATHOPHYSIOLOGY OF LACTICACIDOSIS
Lactic acidosis occurs whenever there is Increased lactic
acid production and decreased utilization
Types and causes of Lactic acidosis
1. Types A (hypoxic)
2. Types B (metabolic)
17.
Type A
Due to hypoxia in tissues (most common)
Hypoxia causes impaired oxidative phosphorylation and
decreased ATP synthesis
To survive ,the cells switch to anaerobic glycolysis for
ATP synthesis
This produces lactate as a final product
The amount of oxygen required to recover oxygen
deficiency (Hypoxia) is called oxygen debt
18.
Type Ais due to inadequate oxygen delivery in tissues
Myocardial infarction
Pulmonary embolism
Tissue hypoperfusion( shock, cardiac arrest)
Increased tissue demand (exercise, seizures, sepsis)
19.
Type B
Due to disorders in carbohydrate metabolism
― Congenital lactic acidosis is due to deficiency of
pyruvate dehydrogenase enzyme
Chronic hepatic disease a company by shock or bleeding
Drug intoxication(ethanol, salicylate)
Combination
Malignancy, Diabetes, Alcohol , HIV and Thiamine deficiency
20.
General malaise
Loss of weight and loss of appetite
Weakness and fatigue
Nausea, and vomiting
Tachypnoea
Tachycardia
SIGNS AND SYMPTOMS
SODIUM BICARBONATE
Sodiumbicarbonate: May worsen oxygen delivery ,increase
lactate production especially in hypoxia induced glycolysis
The surviving sepsis campaign recommended hold sodium
bicarbonate unless profound lactic acidosis and academia (
arterial pH less than 7.1 and serum bicarbonate 6meq/L or
less)
24.
ALTERNATIVES TO BICARBONATE
THERAPY
Tromethamine (tris-hydroxymethyl aminomethane also
called THAM, TRIS and TROMETAMOL
Carbicarb
Dichloroacetate (DCA)
None of these alternative agents have shown benefit in
pts with lactic acidosis
25.
TRIS HYDROXYMETHYL AMINOMETHANE
(THAM)
It is weak alkali and has a benefit over bicarbonate as it
produce less CO2
Clinical trails do not prove THAM to be more effective
than bicarbonate
26.
CARBICARB
It isan equimolar combination of sodium carbonate and
sodium bicarbonate that produce less CO2 than sodium
bicarbonate alone
Trials have not proven any reduction in mortality and
morbidity
27.
DICHLOROACETATE
It isan activator of pyruvate dehydrogenase
It can lower conc: of lactic acid in pts by improving the
lactate utilization
When used in large clinical trail it did not have any effect
on mortality
DCA helpful in lactic acidosis in children with severe
malaria
28.
HAEMODIALYSIS
It israrely indicated as a treatment for lactic acidosis
It is used in drug toxicity ( Metformin induced lactic
acidosis)to speed up elimination of drug/toxin
It is helpful when fluid overload and cardiac or renal
insufficiency is present