Hemostasis and BloodCoagulation
Theory lecture: 1 Systemic Physiology
Dr. Harseen M. Rahim
2.
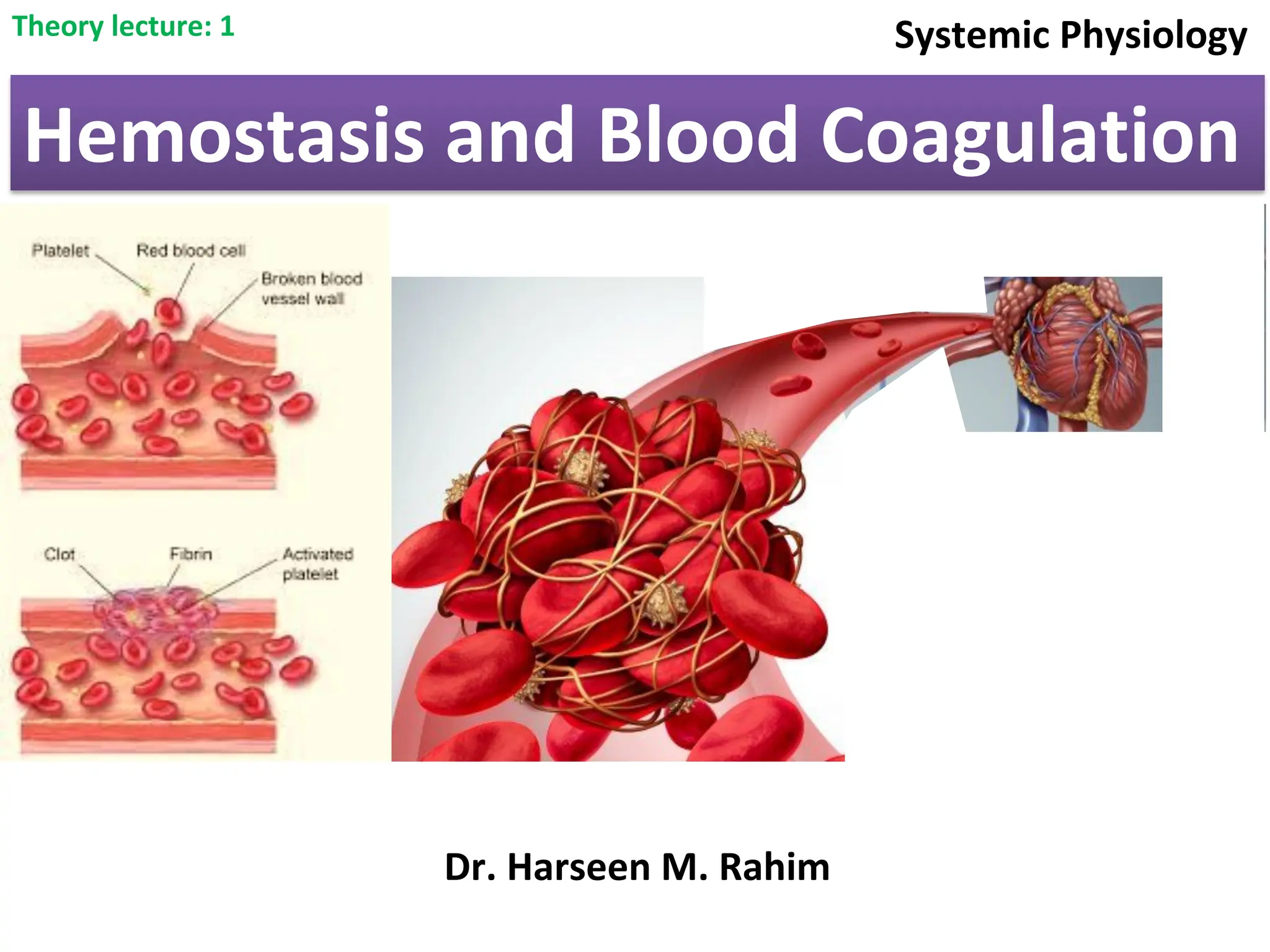
Hemostasis is themechanism that prevent spontaneous blood loss from a
damaged blood vessel and stops hemorrhage by formation of a “plug” that closes
up the damaged site of the blood vessel controlling the bleeding.
Hemostasis
Hemostasis facilitates a series of enzymatic activations that lead to the
formation of a clot with platelets and fibrin net. This clot seals the
injured area, controls and prevents further bleeding while the tissue
regeneration process takes place.
Once the injury starts to heal, the plug slowly remodels, and it dissolves
with the restoration of normal tissue at the site of the damage
3.
(1) Vascular constriction.
Stagesof hemostasis
(2) Formation of a platelet plug
(3) Formation of a blood clot as a result of blood
coagulation.
(4) Growth of fibrous tissue into the blood clot to close the
hole in the vessel permanently.
4.
1- Vascular Constriction:
Immediatelyafter a blood vessel has been cut or ruptured, the
trauma to the vessel wall itself causes the smooth muscle in the
blood vessel wall to contract; this rapidly reduces blood blow
from the ruptured vessel.
For the smaller vessels, the platelets are responsible for much
of the vasoconstriction by releasing a vasoconstrictor substance
known as thromboxane A2.
The spasm can last for many minutes or even hours, during which
time the processes of platelet plugging and blood coagulation can
take place.
5.
2- Formation ofthe Platelet Plug:
If the cut in the blood vessel is very small: many very small vascular holes might
develop throughout the body each day. The cut is often sealed by a platelet plug,
rather than by a blood clot. To understand this, it is important that we first
discuss the nature of platelets themselves.
Normal concentration of platelets in the human blood is between 150,000
and 300,000 per microliter of blood. In animals, it differ according to animal
species.
There are various active factors in the cytoplasm of platelets, including:-
A- contractile proteins that can cause the platelets to
contract.
B- Endoplasmic reticulum and the Golgi apparatus that produce various
enzymes, and especially store large quantities of calcium ions.
6.
C- Mitochondria andenzyme systems that are able to form adenosine
triphosphate (ATP) and adenosine diphosphate (ADP).
D- Enzyme systems that synthesize prostaglandins, that cause many vascular
and other local tissue reactions
E- Fibrin-stabilizing factor stabilizing fibrin networks at the site of injury and thus
preventing premature fibrinolysis.
F- Growth factor that causes vascular endothelial cells, vascular smooth muscle
cells, and fibroblasts to multiply and grow, thus causing cellular growth that
eventually helps repair damaged vascular walls.
7.
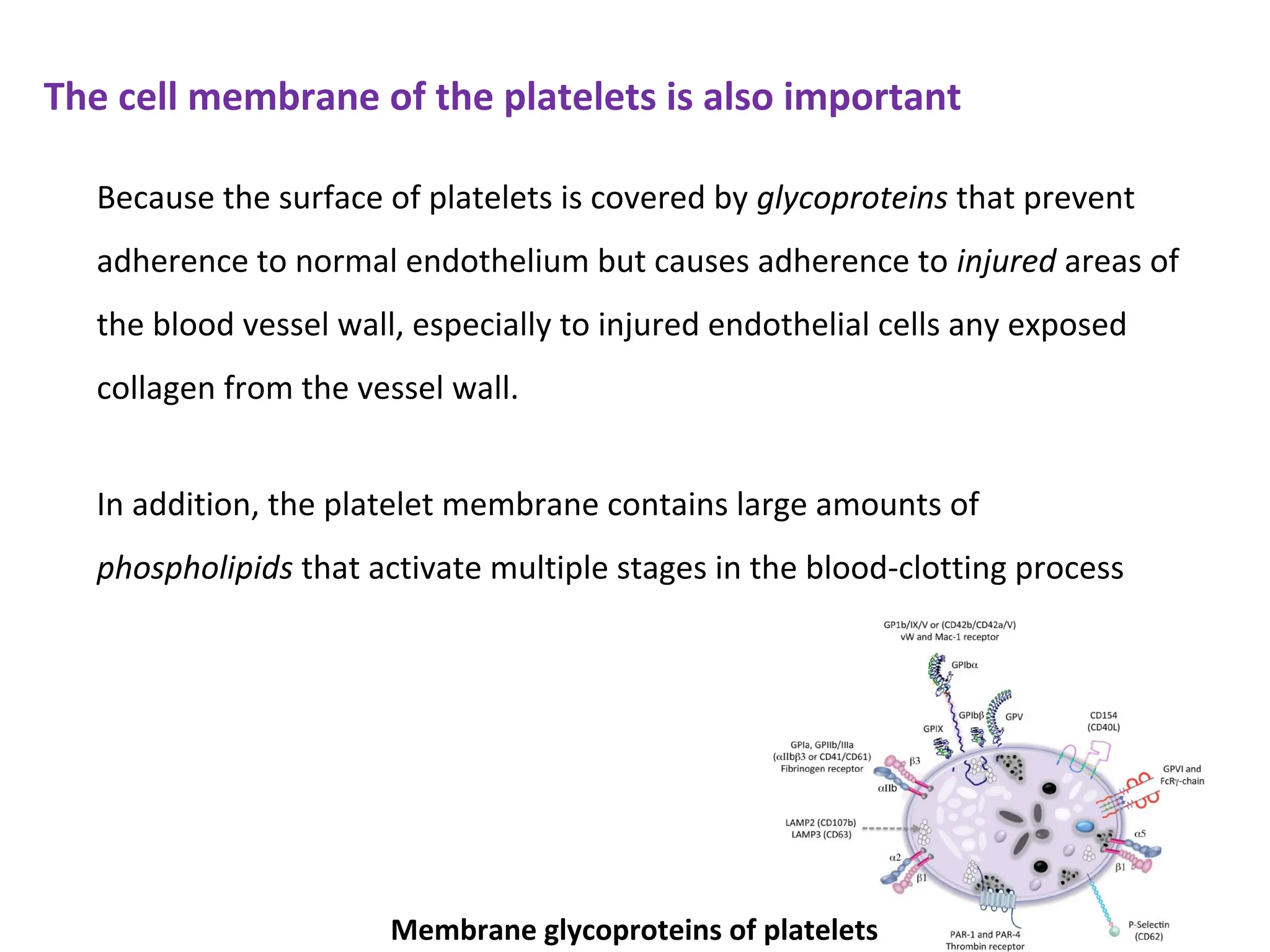
The cell membraneof the platelets is also important
Because the surface of platelets is covered by glycoproteins that prevent
adherence to normal endothelium but causes adherence to injured areas of
the blood vessel wall, especially to injured endothelial cells any exposed
collagen from the vessel wall.
In addition, the platelet membrane contains large amounts of
phospholipids that activate multiple stages in the blood-clotting process
Membrane glycoproteins of platelets
8.
• Swelling andprotruding numerous pseudopods from their surfaces.
Mechanism of the Platelet Plug
When platelets come in contact with a damaged vascular wall, the platelets
themselves immediately begin to:
• they secrete large quantities of ADP; and their enzymes form thromboxane A2.
The ADP and thromboxane in turn act on nearby platelets to activate them, and
the stickiness of these additional platelets causes them to adhere to the original
activated platelets.
• they become sticky so that they adhere to collagen in the tissues and to a
protein called von Willebrand factor that leaks into the traumatized tissue
from the plasma.
• Their contractile proteins contract forcefully and cause the release of granules
that contain multiple active factors.
9.
3- Blood Coagulationin the Ruptured Vessel
Formation of the blood clot begins to develop in 15 to 20 seconds if the
trauma to the vascular wall has been severe, and in 1 to 2 minutes if the
trauma has been minor.
Activator substances from the damaged vascular wall, platelets, and blood
proteins that adhere to the damaged vascular wall can initiate the clotting
process.
If the vessel opening is not too large, the entire broken end of the vessel is
filled with clot within 3 -6 minutes after rupture of a vessel.
After 20 minutes to 1 hour, the clot retracts by platelet function; which
cause further closure of the damaged vessel wall.
10.
4- Fibrous Organizationor Dissolution of the Blood Clot
Once a blood clot has formed, it can follow one of the following pathway:
Conversely, when excess blood has leaked into the tissues and tissue clots have
occurred where they are not needed, special substances within the clot itself
usually become activated. These function as enzymes to dissolve the clot.
(1) It can become invaded by fibroblasts, which subsequently form
connective tissue all through the clot.
(2) it can dissolve.
The usual development for a clot that forms in a small hole of a vessel wall is
invasion by fibroblasts, beginning within a few hours after the clot is formed
(which is stimulated at least partially by growth factor secreted by platelets). This
continues to complete organization of the clot into fibrous tissue within about 1
to 2 weeks.
11.
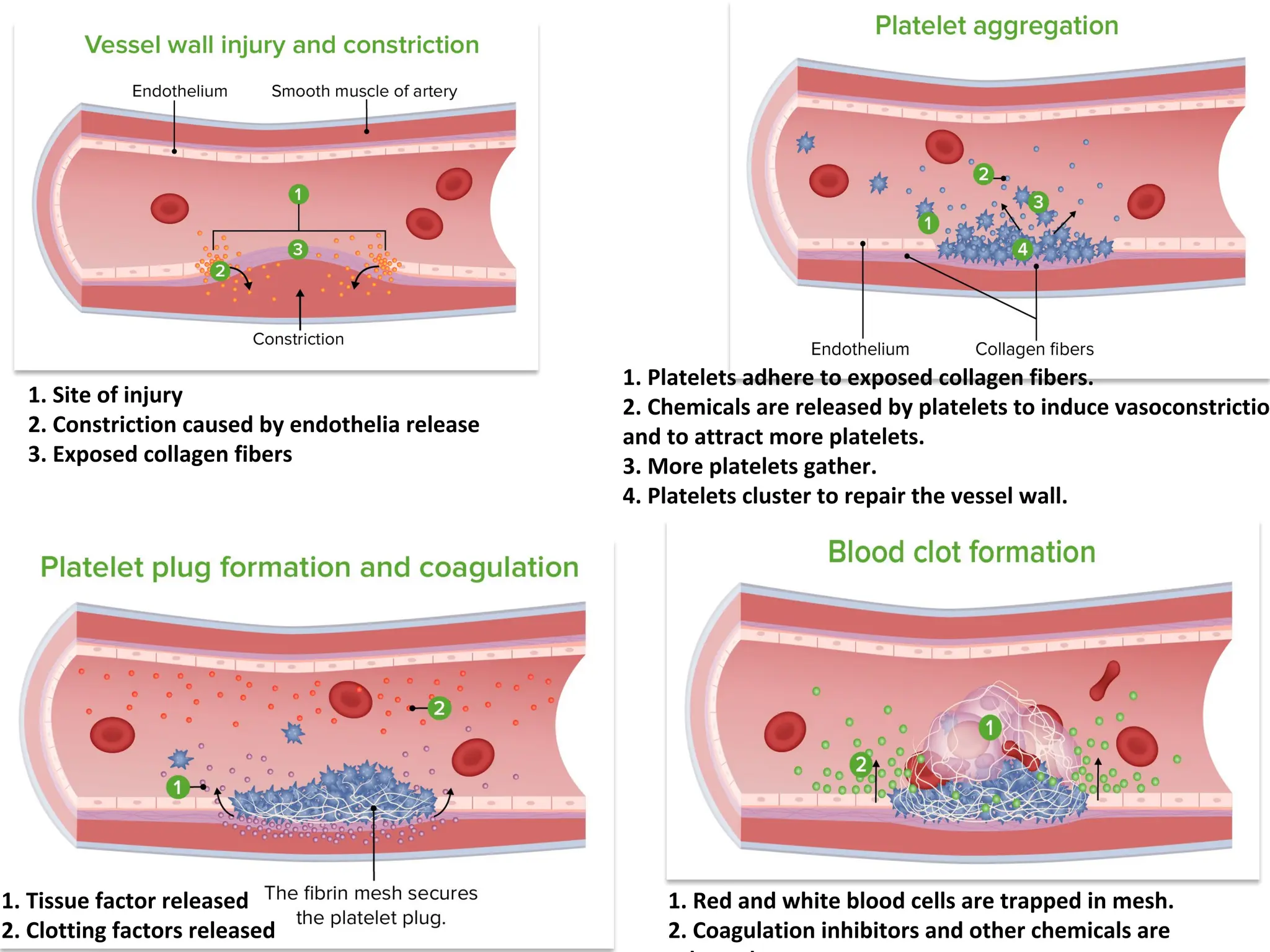
1. Platelets adhereto exposed collagen fibers.
2. Chemicals are released by platelets to induce vasoconstriction
and to attract more platelets.
3. More platelets gather.
4. Platelets cluster to repair the vessel wall.
1. Red and white blood cells are trapped in mesh.
2. Coagulation inhibitors and other chemicals are
1. Site of injury
2. Constriction caused by endothelia release
3. Exposed collagen fibers
1. Tissue factor released
2. Clotting factors released
12.
Coagulation pathway
Basic Theory:
Bloodcoagulation depends on the balance between two groups of
substances: some of them promote coagulation, known as procoagulants,
while others inhibit coagulation, known as anticoagulants.
In the blood stream, the anticoagulants normally predominate, therefore
blood does not coagulate.
However, when a vessel is ruptured, procoagulants from the area of tissue-
damage become “activated”, and then a clot is formed.
13.
1- Formation ofprothrombin activator: in response to rupture of the vessel or
damage to special substances in the blood.
2- Conversion of prothrombin into thrombin by prothrombin activator, in the
presence of sufficient amounts of calcium ion.
3- The thrombin acts as an enzyme to convert fibrinogen into long fibrin fibers
that trap platelets, blood cells, and plasma to form the clot.
There are 3 main steps of blood coagulation (clotting):-
Thrombin also activates the fibrin-stabilizing factor in the plasma, released from
platelets entrapped in the clot, to operates as an enzyme to cause covalent bonds
between more fibrin molecules, as well as multiple cross linkages between
adjacent fibrin fibers.
14.
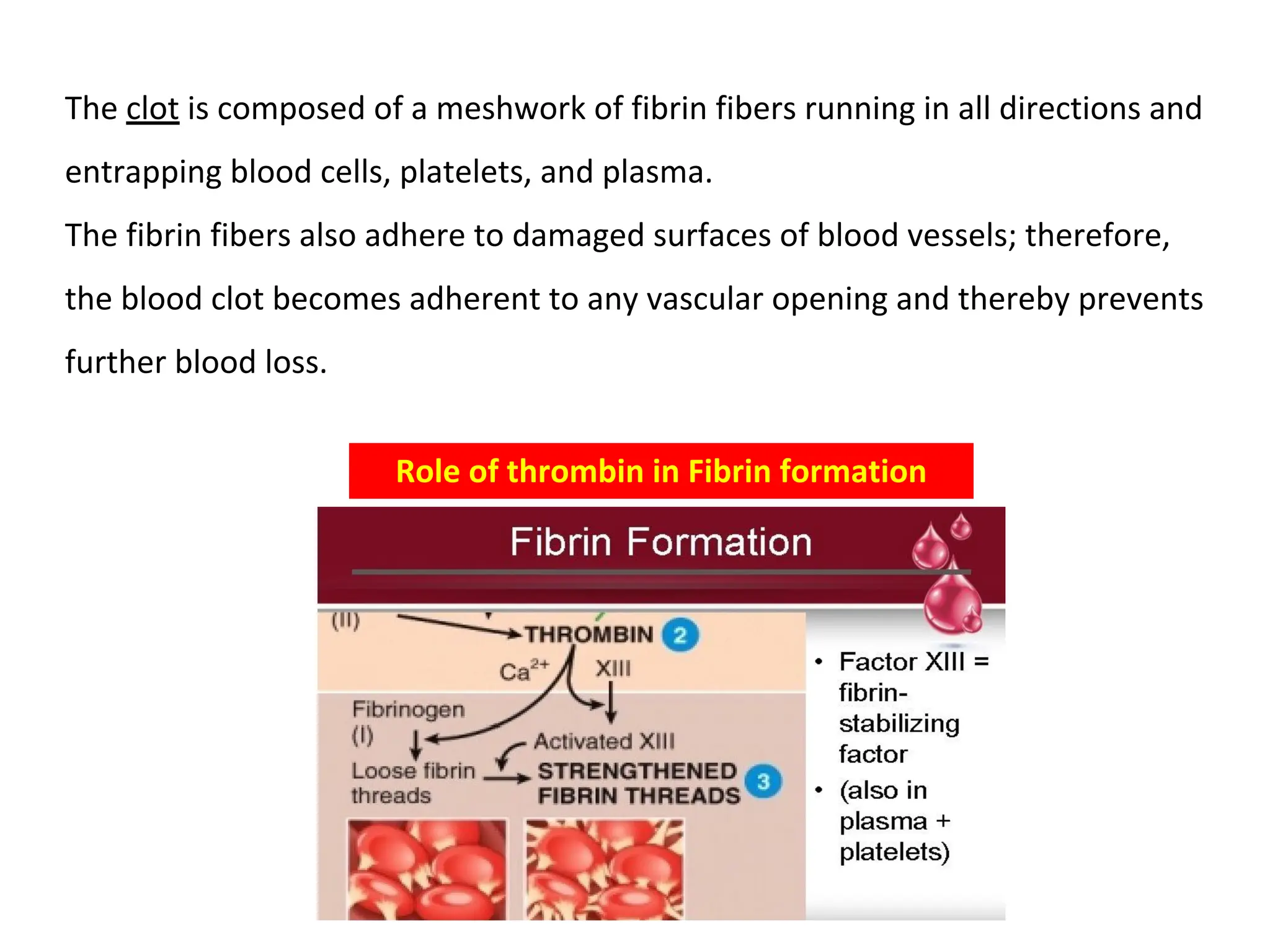
Role of thrombinin Fibrin formation
The clot is composed of a meshwork of fibrin fibers running in all directions and
entrapping blood cells, platelets, and plasma.
The fibrin fibers also adhere to damaged surfaces of blood vessels; therefore,
the blood clot becomes adherent to any vascular opening and thereby prevents
further blood loss.
15.
Prothrombin is aprotein that present in normal plasma in a concentration of
about 15 mg/dl. Prothrombin is formed continually by the liver, and it is
continually being used throughout the body for blood clotting.
Liver failure or diseases prevent normal prothrombin formation, the
concentration of prothrombin in the plasma markedly reduced to provide
normal blood coagulation.
Prothrombin and Thrombin
Vitamin K is required by the liver for normal formation of prothrombin as
well as other clotting factors. Therefore, either vitamin K-deficiency or
presence of liver disease can decrease the prothrombin level and bleeding
tendency results.
16.
Mechanisms that initiateclotting
The mechanism of clot formation (coagulation) involves formation
of prothrombin activator by:
(1) Trauma to the vascular wall and adjacent tissues.
(2) Trauma to the blood.
(3) Contact of the blood with damaged endothelial cells or with collagen and
other tissue elements outside the blood vessel.
Prothrombin activator is formed in two ways:
1) Extrinsic pathway that begins with trauma to the vascular wall and
surrounding tissues.
2) Intrinsic pathway that begins in the blood itself.
17.
In both theextrinsic and the intrinsic pathways, a series of different plasma
proteins called blood clotting factors play major roles. Most of these are inactive
forms of enzymes. When converted to the active forms, their enzymatic actions
cause the successive, cascading reactions of the clotting process.
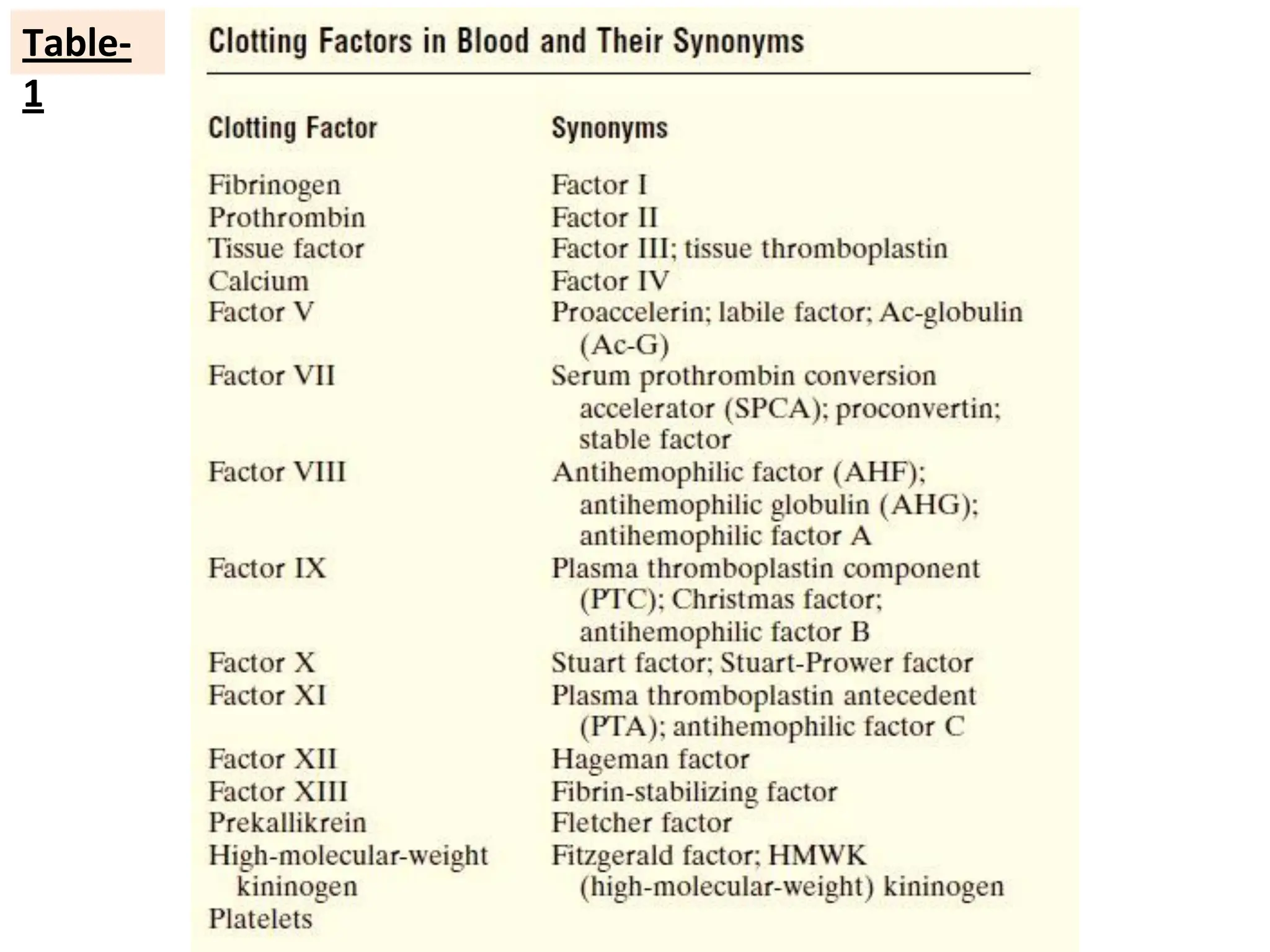
Most of the clotting factors are listed in Table-1, are designated by Roman
numerals. To indicate the activated form of the factor, a small letter “a” is
added after the Roman numeral, such as Factor VIIIa to indicate the activated
state of Factor VIII.
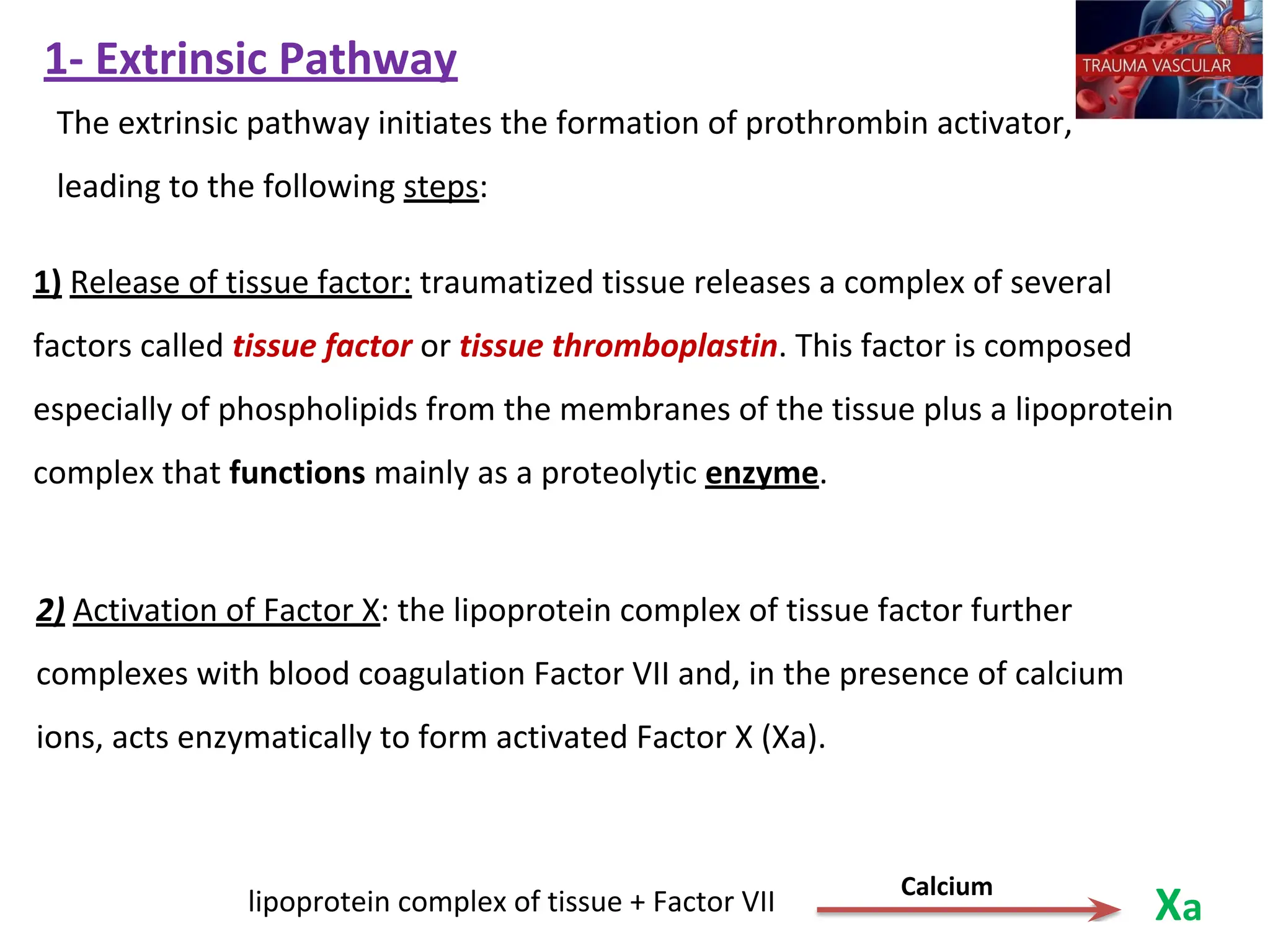
1- Extrinsic Pathway
1)Release of tissue factor: traumatized tissue releases a complex of several
factors called tissue factor or tissue thromboplastin. This factor is composed
especially of phospholipids from the membranes of the tissue plus a lipoprotein
complex that functions mainly as a proteolytic enzyme.
The extrinsic pathway initiates the formation of prothrombin activator,
leading to the following steps:
2) Activation of Factor X: the lipoprotein complex of tissue factor further
complexes with blood coagulation Factor VII and, in the presence of calcium
ions, acts enzymatically to form activated Factor X (Xa).
lipoprotein complex of tissue + Factor VII
Calcium
Xa
20.
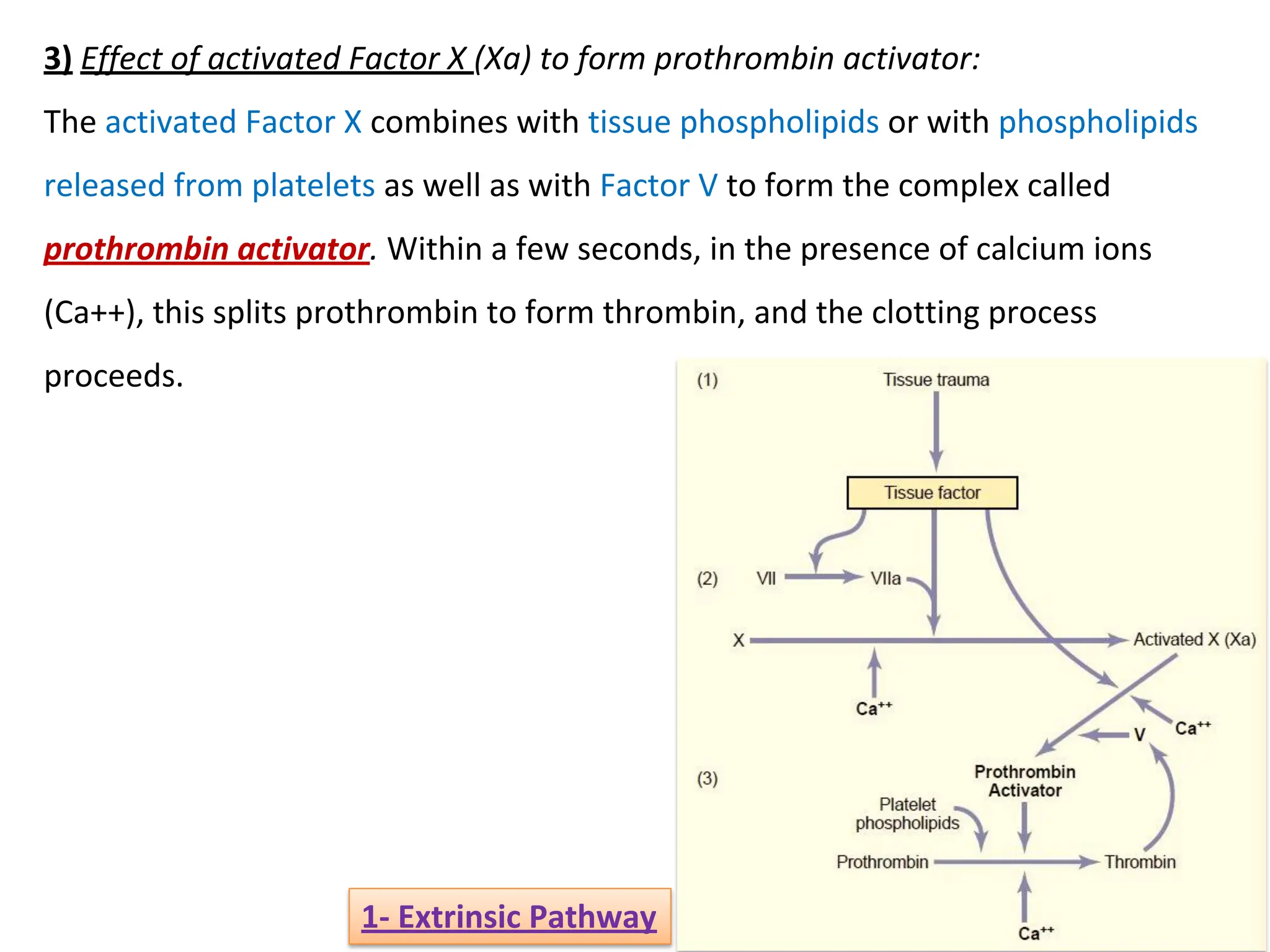
3) Effect ofactivated Factor X (Xa) to form prothrombin activator:
The activated Factor X combines with tissue phospholipids or with phospholipids
released from platelets as well as with Factor V to form the complex called
prothrombin activator. Within a few seconds, in the presence of calcium ions
(Ca++), this splits prothrombin to form thrombin, and the clotting process
proceeds.
1- Extrinsic Pathway
21.
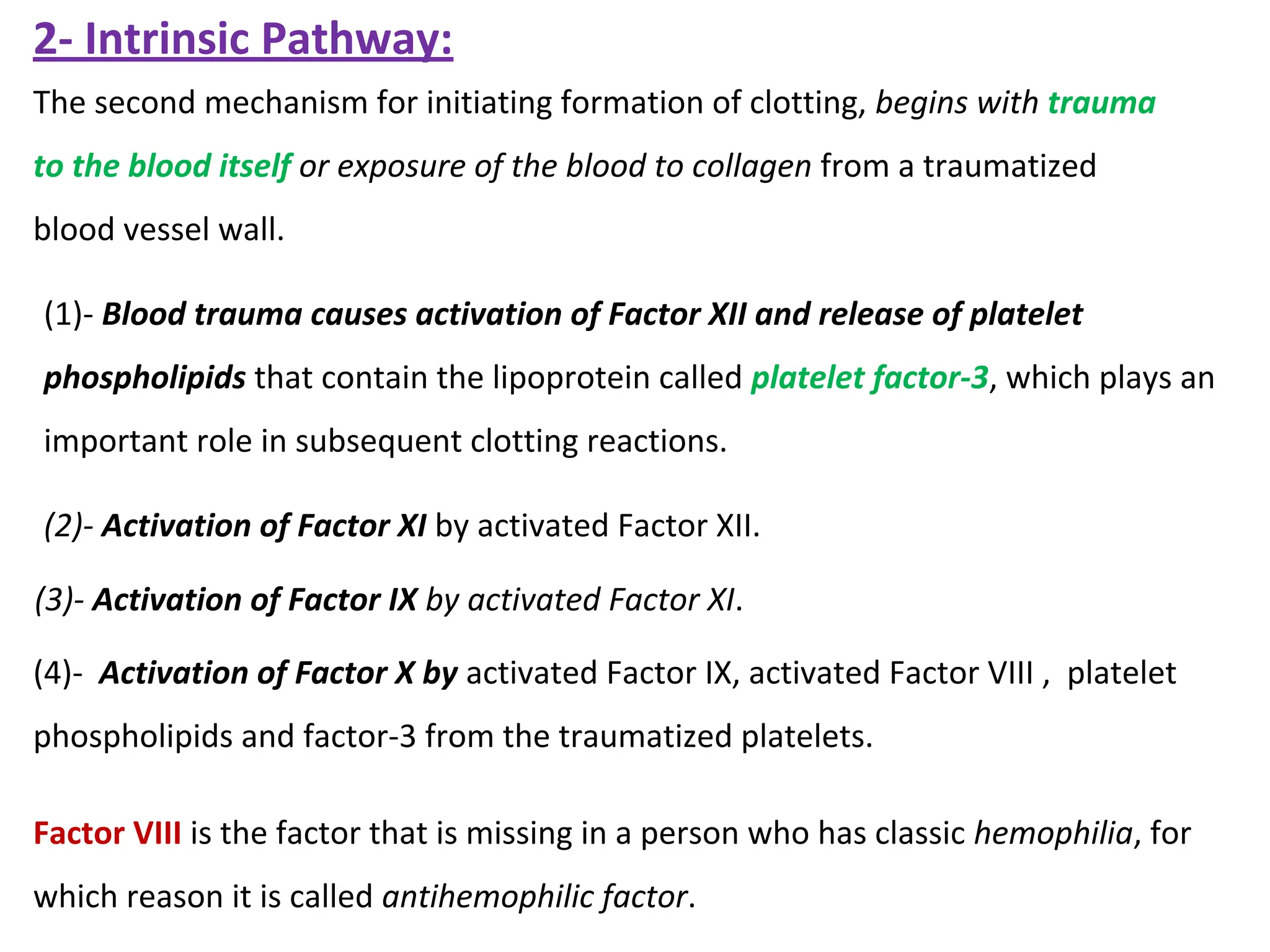
(2)- Activation ofFactor XI by activated Factor XII.
(3)- Activation of Factor IX by activated Factor XI.
(4)- Activation of Factor X by activated Factor IX, activated Factor VIII , platelet
phospholipids and factor-3 from the traumatized platelets.
Factor VIII is the factor that is missing in a person who has classic hemophilia, for
which reason it is called antihemophilic factor.
(1)- Blood trauma causes activation of Factor XII and release of platelet
phospholipids that contain the lipoprotein called platelet factor-3, which plays an
important role in subsequent clotting reactions.
The second mechanism for initiating formation of clotting, begins with trauma
to the blood itself or exposure of the blood to collagen from a traumatized
blood vessel wall.
2- Intrinsic Pathway:
22.
2- Intrinsic
Pathway:
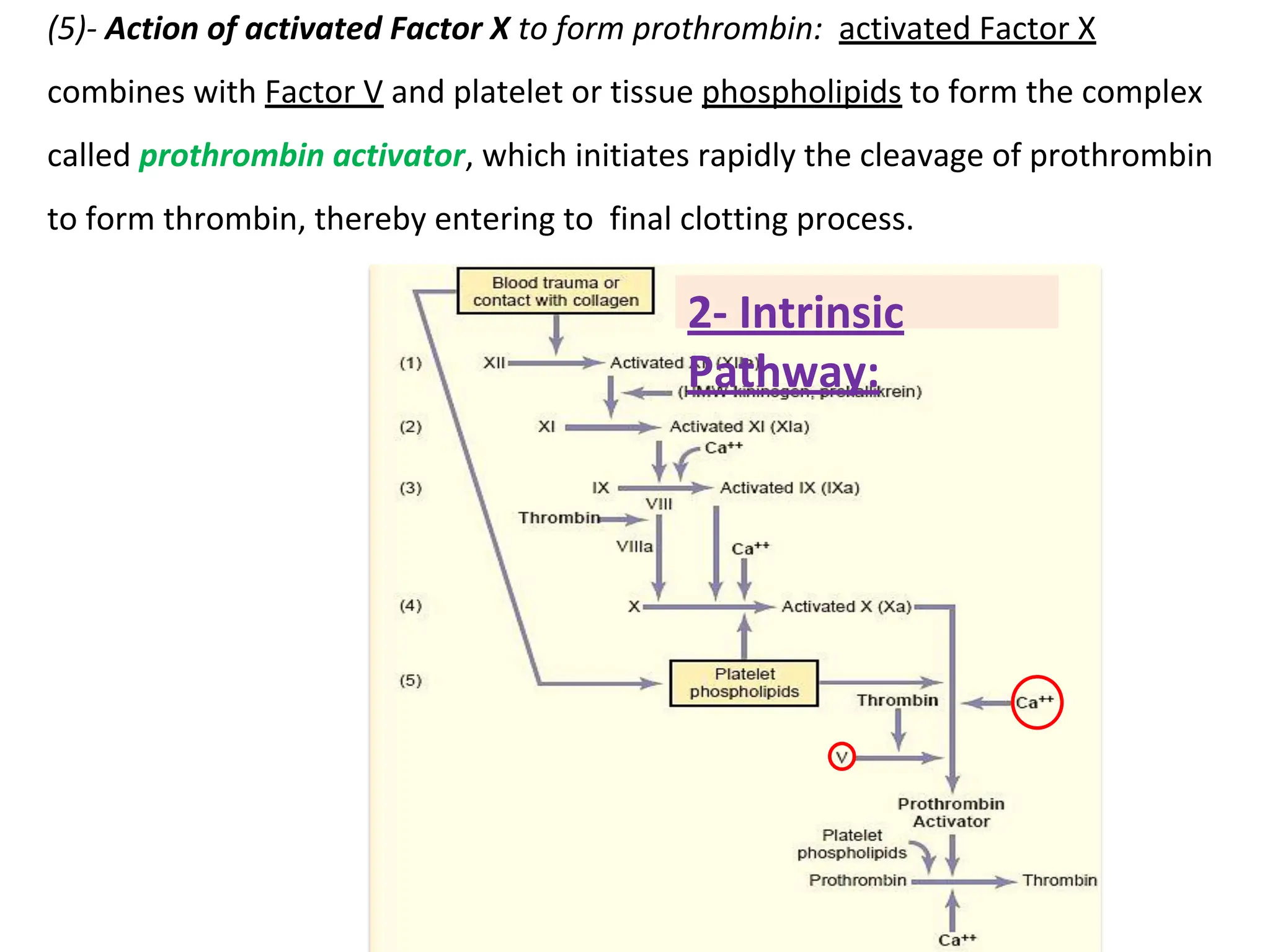
(5)- Actionof activated Factor X to form prothrombin: activated Factor X
combines with Factor V and platelet or tissue phospholipids to form the complex
called prothrombin activator, which initiates rapidly the cleavage of prothrombin
to form thrombin, thereby entering to final clotting process.

































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



