Downloaded 190 times
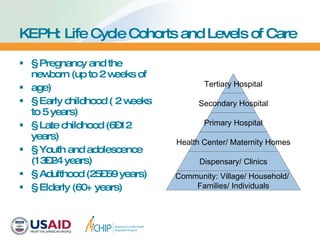

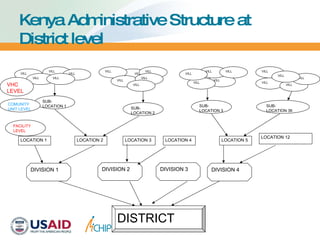
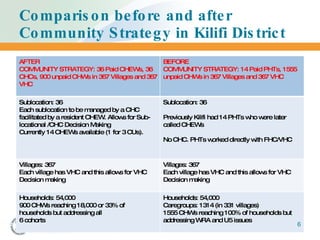
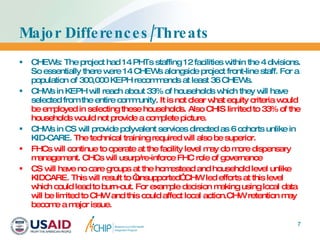

The Kenya Essential Package for Health (KEPH) introduced a comprehensive community health strategy aimed at empowering households and communities to improve health care delivery. It segments health services into six life-cycle cohorts and employs trained community health workers to provide care at the household level, supporting enhanced health facility-community linkages. Despite its innovations, challenges remain, such as limited coverage and potential burnout among community health workers due to a lack of support systems.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















