Jurnal pediatric
•Download as DOCX, PDF•
0 likes•20 views

This study evaluated the safety and efficacy of a protocol-defined transplacental treatment for fetal supraventricular tachycardia (SVT) and atrial flutter (AFL). 50 pregnant women with fetuses diagnosed with sustained SVT or AFL between 22-37 weeks gestation were enrolled across 15 institutions in Japan from 2010-2017. The primary treatment protocol involved digoxin, sotalol, or flecainide administered until delivery. Fetal tachyarrhythmia resolved in 89.8% of cases overall and 75% of cases with fetal hydrops. However, serious adverse events occurred in 1 mother and 4 fetuses, resulting in discontinuation of treatment in 4 patients. Two fetal deaths occurred

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Jurnal pediatric
Similar to Jurnal pediatric (20)
More from dr. andrea wahyu
Recently uploaded
Recently uploaded (20)
Jurnal pediatric
- 1. J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 4 , N O . 7 , 20 1 9 ª 2 0 19 B Y T H E A M ERI C AN C OLLEGE OF CA RD IOLOGY F O U N D A T I O N P U BL I S H E D B Y E L S E V I E R Antenatal Therapy for Fetal Supraventricular Tachyarrhythmias Multicenter Trial Takekazu Miyoshi, MD, a Yasuki Maeno, MD, b, * Toshimitsu Hamasaki, PHD, c Noboru Inamura, MD, d Satoshi Yasukochi, MD,e Motoyoshi Kawataki, MD,f Hitoshi Horigome, MD,g Hitoshi Yoda, MD,h Mio Taketa zu, MD,i Masaki Nii, MD, j Akiko Hagiwara, MD, k Hitoshi Kato, MD, l Wataru Shimizu, MD, m Isao Shiraishi, MD, n Heima Sakaguchi, MD, n Keiko Ueda, MD, a Shinji Katsuragi, MD, a Haruko Yamamoto, MD, o Haruhiko Sago, MD, p Tomoaki Ikeda, MD, q, * on behalf of the Japan Fetal Arrhythmia Group ABSTRACT BACKGROUND Standardized treatment of fetal tachyarrhythmia has not been established. OBJECTIVES This study sought to evaluate the safety and efficacy of protocol-de fined transplacental treatment for fetal supraventricular tachycardia (SVT) and atrial flutter (AFL). METHODS In this multicenter, single-arm trial, protocol-defined transplacental treatment using digoxin, sotalol, and flecainide was performed for singleton pregnancies from 22 to <37 weeks of gestation with sustained fetal SVT or AFL $180 beats/min. The primary endpoint was resolution of fetal tachyarrhythmia. Secondary endpoints were fetal death, pre-term birth, and neonatal arrhythmia. Adverse events (AEs) were also assessed. RESULTS A total of 50 patients were enrolled at 15 institutions in Japan from 2010 to 2017; short ventriculoatrial (VA) SVT (n ¼ 17), long VA SVT (n ¼ 4), and AFL (n ¼ 29). One patient with AFL was excluded because of withdrawal of consent. Fetal tachyarrhythmia resolved in 89.8% (44 of 49) of cases overall and in 75.0% (3 of 4) of cases of fetal hydrops. Pre-term births occurred in 20.4% (10 of 49) of patients. Maternal AEs were observed in 78.0% (39 of 50) of patients. Serious AEs occurred in 1 mother and 4 fetuses, thus resulting in discontinuation of protocol treatment in 4 patients. Two fetal deaths occurred, mainly caused by heart failure. Neonatal tachyarrhythmia was observed in 31.9% (15 of 47) of neonates within 2 weeks after birth. CONCLUSIONS Protocol-defined transplac ental treatme nt for fetal SVT and AFL was effe ctive and tolerable in 90% of patients. However, it should be kept in mind that serious AEs may take place in fetuses and that tachy- arrhythmias may recur within the first 2 weeks after birth. (J Am Coll Cardiol 2019;74:874–85) © 2019 by the American College of Cardiology Foundation. Listen to this manuscript’ s audio summary by Editor-in- Chief Dr. Valentin Fuster on JACC.or g. From the a Department of Perinatology and Gynecology, National Cerebral and Cardiovascular Center, Suita, Japan; b Department of Pediatrics and Child Health, Kurume University School of Medicine, Kurume, Japan; c Department of Data Science, National Cerebral and Cardiovascular Center, Suita, Japan; d Department of Pediatric Cardiology, Osaka Women’s and Children’s Hospital, Izumi, Japan; e Department of Cardiology, Nagano Children’s Hospital, Azumino, Japan; f Department of Gynecology and Obstetrics, Tohoku University Graduate School of Medicine, Sendai, Japan; g Department of Pediatrics, University of Tsukuba, Tsukuba, Japan; h Department of Neonatology, Toho University Omori Medical Center, Tokyo, Japan; i Department of Pediatric Cardiology, Saitama Medical University International Medical Center, Hidaka, Japan; j Department of Cardiology, Shizuoka Chil- dren’s Hospital, Shizuoka, Japan; k Department of Internal Medicine, Kanagawa Children’s Medical Center, Yokohama, Japan; l Department of Pediatric Cardiology, National Center for Child Health and Development, Tokyo, Japan; m Department of Cardiovascular Medicine, Nippon Medical School, Tokyo, Japan; n Department of Pediatric Cardiology, National Cerebral and Cardiovascular Center, Suita, Japan; o Department of Advanced Medical Technology Development, National Cerebral and Cardiovascular Center, Suita, Japan; p Center for Maternal-Fetal, Neonatal and Reproductive Medicine, National Center for Child Health and Development, Tokyo, Japan; and the q Department of Obstetrics and Gynecology, Mie University, Tsu, Japan. *Drs. Maeno and Ikeda contributed equally to this work. This work was supporte d by the Agency for Medical Research and Develop- ment of the Ministry of Education, Culture, Sports, Science, and Technology of Japan (JP15lk0201001). The funding organization had no role in the trial design; data collection, analysis, or interpretation; or manuscript preparation. All authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received January 18, 2019; revised manuscript received June 5, 2019, accepted June 10, 2019. ISSN 0735-1097/$36.00 https://doi.org/10.1016/j.jacc.2019.06.024
- 2. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 875 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 875 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 Fetal tachyarrhythmia develops in <0.1% of pregnancies. The most common forms of fetal tachya rr hy thm ia include suprave ntric ula r tachycardia (SVT) and atrial flutter (AFL) (1). Although many cases are of minor clinical signifi- cance, fast or long-lasting tachyarrhythmias often cause fetal heart failure and fetal hydrops (1,2). Without treatment, hydrops is found in 30% to 40% of fetuses with SVT and in 7% to 43% of fetuses with AFL (3,4). For fetuses with hydrops, elective pre-term delivery and other lifesaving interventions are often attempted, but perinatal mortality is signif- icantly highe r than in fetuse s without hydrops (3–5). Availa ble data sugge st that the risk of fetal death P R O C E D U RE S. The study design was described previously (9). Inclusion criteria were as follows: 1) sustained fetal tachyarrhythmia $180 beats/min, with a diagnosis of SVT or AFL (fetal tachyar- rhythmia is defined as sustained when present $50% during a 40-min fetal heart rate monitoring or a 30-min echocardiogra- phy sessio n); 2) 22 to <37 weeks of gestation; 3) singleton pregnancy; and 4) patients’ written consent to study participation. Exclusion criteria were as follows: 1) the pa- tient had mental or psychiatric conditions that prec lud e safe study partic ipa tio n; 2) the A B B R E V I A T I O N S A N D A C R O N Y M S AE = adverse event AFL = atrial flutter AV = atriovent ricu lar AVRT = atriovent ricular re-entran t tachycardia CI = confidence interval EAT = ectopic atrial tachycard ia SVT = supravent ricu l ar tachycard ia VA = ventriculoatrial will be higher if tachyarrhythmia is left untreated in fetal hydrop s. S EE P AGE 8 8 6 Before designing this clinical trial, we conducted a nationwide survey of fetal tachyarrhythmia in Japan from 2004 to 2006 (6). A total of 82 fetuses were analyzed, of whom 41 received in utero treatment. Transpla c e ntal treatme nt was fairly effe c tiv e in 90.2% (37 of 41) of cases and in 81.8% (9 of 11) of cases with fetal hydrops. These findings were comparable to those of previous reports (2–4,7). Although several retrospective studies have supported the efficacy of transplacental treatment for fetal SVT and AFL, the choice of first-line and second-line antiarrhythmic therapy remains controversial (8). Because most studies are confounded by physician and institutional preferences, there are few data supporting specific treatment protoc ols. The primary goal of this study was to evaluate the safety and efficacy of protocol-defined transplacental treatment for fetal SVT and AFL. We conducted a multic e nte r single -a r m trial. MET HODS S T U DY D E S IG N A N D P A RT ICIP A N TS. This study was a multicenter, single-arm trial. The study protocol was approved by the Institutional Review Board of the National Cerebral and Cardiovascular Center of Japan in July 2010 (M20-045). Patient enrollment began in October 2010. This study was conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from the patients. This trial was registered in the University Hospital Medical Information Network Clinical Trials Registry as UMIN000004270. The Independent Safety Evalu- ation Committee was responsible for the overall safe ty of this trial. patient was anticipated to have contraindications to the antiarrhythmic medications used in the study; 3) serious, life-threatening malformations were diag- nosed in the fetus; 4) the fetus was diagnosed with multifocal atrial tachycardia or chaotic atrial tachy- cardia; and 5) the patient or fetus was not eligible, in the investigator’s judgment, for this clinical study for other reasons. Fetal tachyarrhythmias were diagnosed using pulsed wave Doppler echocardiography and M-mode recordings (9). Fetuses with multiple arrhythmias were classified according to the dominant mecha- nism. Fetal hydrops was characterized by the pres- ence of subcutaneous edema in addition to at least 1 of the following findings: ascites, pleural effusion, and pericardial effusion (10). All fetal ultrasound scans were reviewed by the Protocol Evaluation Committee. Recruiting centers were as follows: National Cere- bral and Cardiovascular Center, Kurume University School of Medicine, Osaka Women’s and Children’s Hospital, National Center for Child Health and Development, Kanagawa Children’s Medical Center, University of Tsukuba, Toho University Omori Medi- cal Center, Hokkaido University, Hyogo Prefectural Children’s Hospital, Nagano Children’s Hospital, Shizuoka Children’s Hospital, Kobe City Medical Center General Hospital, Mie University, Okayama Medical Center, and Osaka Univer sity, all in Japan. TRA N S P L A CE N TA L TRE A TME N T P ROTO CO L . Proto- col-defined treatment with digoxin, sotalol, or fle- cainide was continued until delivery (9). Ineffective fetal therapy was defined as therapy that did not resolve fetal tachyarrhythmia or when fetal death was strongly suspected because of progression of fetal hydrops. If the investigator judged that the preg- nancy could not be maintained to term, the woman was delivered of the fetus. When maternal or fetal adverse events (AEs) secondary to antiarrhythmic
- 3. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 876 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 876 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 Analysis for maternal outcome (n = 50) excluded from analysis (n = 0) Analysis for fetal outcome (n = 49) excluded from analysis (n = 1) • consent withdrawal (n = 1) Analysis for neonatal outcome (n = 47) excluded from analysis (n = 2) • fetal death (n = 2) F IGUR E 1 Trial Profile Screened (n = 88) Registered (n = 50) Fetal treatment Declined or ineligible (n = 38)* For fetuses with short ventriculoatrial (VA) SVT or AFL without hydrops, digoxin was the first-line ther- apy. Rapid initial saturation was performed with a 0.5- mg intrav en ous injection. Intra ve no us injections of 0.25 mg were administered at 8 and 16 h after the initial dose. If intravenous injections were not feasible, oral digoxin (1.5 mg/day) was given in 3 divided doses. Subse que ntly, oral digoxin at 0.75 mg/day was given in 3 divided doses, with adjustment to maintain maternal serum concentra- tions from 1.5 to 2.0 ng/ml. If fetal therapy was inef- fective 3 days after establishing the target serum digoxin conc e ntra tion, the investiga tor move d to the second-line therapy. Sotalol at 160 mg/day in 3 divided based on the protocol (n = 50) Consent withdrawal (n = 1) doses was adde d. If a regim e n of 3 days of treatment at 160 mg/da y of sotalol was ineffe ctive, the patient then proc e e de d to 240 mg/da y in 2 divided doses. If 240 mg/da y was ineff e ctive afte r 3 days of treatment, the patie nt proc ee d e d to 320 mg/da y in 2 divided doses. If 320 mg/da y was ineff e ctive after 3 days of Primary and secondary outcome at birth (n = 49) Fetal death (n = 2) Secondary outcome at 1-month follow-up after birth (n = 47) Analysis *A total of 31 patients did not meet the inclusion criteria because of nonsusta ine d fetal tachyarrhythmia (n ¼ 16), ventricular tachycardia (n ¼ 5), $37 weeks of gestation (n ¼ 5), twin pregnancy (n ¼ 1), and study participation refusal (n ¼ 4). Seven patients met the exclusion criteria for fetal life-threate ning malformations: Ebstein’s anomaly (n ¼ 4); hypoplastic left heart syndrome (n ¼ 2); and cardiac tumors with ventricular outflow obstruction (n ¼ 1). agents were observed, the investigator could reduce the dosage. Sotalol and flecainide were discontinued if the corrected QT interval was >500 ms. After birth, it was left up to each institution to decide whether to contin ue antia rr hyth m ic agents prophyla ctica lly. treatment, the investigator moved to the third-line therapy. Flecainide was administered at 200 mg/day in 2 divided doses in addition to digoxin. If 200 mg/day was ineffective after 3 days of treatment, the patient proce e de d to 300 mg/da y in 2 divided doses. If 300 mg/day was ineffective after 3 days of treatment, protocol-defined treatment was discontinued. If the fetus had hydrops, fetal therapy started with the second -lin e therapy. For fetuses with long VA SVT, sotalol and flecai- nide were used as first-line and second-line therapy, respectively, regardless of the presence or absence of fetal hydrops. The dosage and administration schedule were the same as those for fetuses with short VA SVT or AFL. E N D P O I N TS. The primary endpoint was resolution of fetal tachyarrhythmia, defined as normal sinus rhythm or mean heart rate of <180 beats/min. Res- olution of fetal tachyarrhythmia was judged by a 40- min fetal heart rate monitoring or 30-min echocar- diography session. Secondary endpoints were fetal death related to tachyarrhythmia, pre-term birth, cesarean section performed as a result of fetal arrhythmia, improvement in heart rate and less edema after fetal therapy, prevalence of neonatal arrhythmia, neonatal central nervous system disor- der, and neonatal survival. Safety endpoints were maternal, fetal, and neonatal AEs. All AEs were assessed by the Independent Safety Evaluation Committee. Because we focused on evaluating the safety of our protocol-defined transplacental treat- ment, we assessed the maternal cardiac condition before and during this treatment by using
- 4. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 877 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 877 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 echocardiography as well as electrocardiography. Maternal serum levels of the antiarrhythmic agents and plasma brain natriuretic peptide levels were also measured. ST A T I ST I CA L A N A L YSIS. Sample size was deter- mined according to the precision-based method. A sample size of 50 produced a 2-sided Clopper-Pearson exact 95% confid en c e interval (CI) with a width of 18.5 when the sample propo rtion was assum e d to be 90%. More details were presented in the protocol paper (9). All statistical analyses were performed ac- cording to a pre-specified statistical analysis plan finalized before database lock and release of data. All analyses were performed using SAS for Windows software version 9.3 (SAS Institute, Cary, North Car- olina). According to the intention-to-treat principle, the primary analysis group was defined as all regis- tered pregnant mothers, fetuses, or neonates. Continuous data were presented as medians and range. Categorical data were presented as frequencies and percentages. For the primary endpoint, the number and percentage of fetuses with resolution of fetal tachyarrhythmia were calculated with a 2-sided Clopper-Pearson exact 95% CI. The primary outcome was also analyzed on the basis of the per-protocol set group to assess the robustness of conclusions from the primary analysis group. The per-protocol set group excluded subjects with major protocol viola- tions or loss to follow -u p. Secondary endpoints were analyzed similar to primary endpoints. The Steel-Dwass test was used to compare continuous variables among 3 subtypes of fetal tachyarrhythmia. A value of p < 0.05 was considered significant in all analyses. For the safety analysis, the number of AEs and the number of sub- jects with AEs were calcu late d acco rdin g to causality. RESULT S STUDY COHORT AND BASELINE CHARACTERISTICS. A total of 50 patients were enrolled and treated at 15 institutions in Japan from Octob er 2010 to January 2017 (Figure 1). During the protocol treatment, 1 pa- tient with AFL was excluded because of withdrawal of consent, thus leaving 49 patients available for anal- ysis of primary and secondary outcomes. Safety endpo ints were assesse d in all 50 patients. Exce pt for 2 fetal deaths, 1-month follow-up was available for 47 neonates. Maternal complications were observed in 7 patients (14.0%): type 2 diabetes mellitus, solitary kidney with mild renal dysfunction, patent ductus arteriosus, history of depression or schizophrenia (n ¼ 1 each) and controlle d hypothy roidis m (n ¼ 2). TAB LE 1 Baseline Charac ter i sti cs Total Short VA SVT Long VA SVT AFL (N ¼ 49) (n ¼ 17) (n ¼ 4) (n ¼ 28) Maternal age, yrs 32 (21–40) 32 (21–39) 35 (31–38) 31.5 (24–40) Primipara status 24 (48.0) 8 (47.1) 2 (50.0) 13 (46.4) Gestational age at 31 (24–36) 27 (24–35)* 32.5 (26–36) 32 (27–35) diagnosis, weeks Atrial rate, beats/min 430 245 230 450 (185–520) (185–280) (192–260) (410–520)† Ventricular rate, beats/min 230 245 230 224.5 (185–280) (185–280) (192–260) (205–260) Fetal hydrops at diagnosis 4 (8.0) 2 (11.8) 1 (25.0) 1 (3.6) Fetal effusion or ascites at diagnosis 19 (38.0) 9 (52.9) 2 (50.0) 8 (28.6) Fetal abnormality ‡ 6 (12.0) 2 (11.8) 2 (50.0) 2 (7.1) Threatened pre-mature labor 10 (20.0) 3 (17.7) 1 (25.0) 6 (21.4) Values are median (range) or n (%). *Significant difference when compared with fetuses with AFL and long VA SVT (p < 0.05, the Steel-Dwass test). †Significant difference when compared with fetuses with short and long VA SVT (p < 0.05, the Steel-Dwass test). ‡Beckwith-Wiedemann syndrome with umbilical hernia (AFL), suspected Costello syndrome with hypoplastic lung (AFL), corrected transposition of the great arteries (AFL), isolated ventricular septal defect (short VA SVT), tuberous sclerosis with cardiac tumors (long VA SVT), and heterotaxy syndrome with severe pulmonary valve stenosis and ventricular septal defect (long VA SVT). AFL ¼ atrial flutter; SVT ¼ supraventricular tachycardia; VA ¼ ventriculoatrial. Obstetrical complications were observed in 12 pa- tients (24.0%): threatened pre-term labor (n ¼ 10), placenta previa (n ¼ 1), and gestational diabetes mellitus (n ¼ 1). Median gestational age at diagnosis was 31 weeks (range 24 to 36 weeks) (Table 1). Only 2 fetuse s (4.0% ) had ventric ula r rates betwee n 180 and 200 beats/min: 1 with short VA SVT and another with long VA SVT. Fetal hydrops at diagnosis of fetal arrhyth mia was observe d in 4 fetuse s (8.0% ; 95% CI: 2.2% to 19.2%). Six fetuses with morphological ab- normalities (12.0%) were not excluded from this study (Online Table 1). Beta-stimulants were used for tocolysis in all 10 patients with threatened pre-term labor but were discontinued before starting the pro- tocol treatment. Fetal hydrops was found in 2 of 10 patients with threatened pre-term labor, and this was not statistically different from the incidence in pa- tients without threa ten e d pre-te r m labor (20.0% vs. 5.0%; difference of 15%; 95%CI: 20.8 to 49.6; Fisher exact test p ¼ 0.17). P RIMA RY A N D SE CO N DA RY O U TCO ME S. Fetal tachyarrhythmia resolved in 44 of 49 patients overall (89.8%; 95% CI: 77.8% to 96.6%) and in 3 of 4 patients with fetal hydrops (75.0%). Two cases of fetal hydrops resolved in utero, and 1 fetus pro- gressed to hydrops, with hydrops present at de- livery in 3 neonates. Median gestational age at birth was 38 weeks (range 29 to 40 weeks). Pre-term births occurred in 7 neonates (14.3%; 95% CI: 5.9% to 27.2%). A total of 22 patients (44.9%; 95% CI: 30.7% to 59.8%) underwent cesarean delivery, but
- 5. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 878 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 878 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 TAB LE 2 Primary and Secondary Outcomes Total Short VA SVT Long VA SVT AFL (N ¼ 49) (n ¼ 17) (n ¼ 4) (n ¼ 28) Final treatment agents Digoxin 26 9 0 17 Sotalol 4 0 4 0 Digoxin and sotalol 15 6 0 9 Digoxin and flecainide 5 2 0 3 Resolution of fetal tachyarrhythmia 44 (89.8) 15 (88.2) 4 (100.0) 25 (89.3) Recurrence in utero 14 (32.6) 7 (43.8) 1 (25.0) 6 (26.1) Duration of treatment, weeks 6 (1–13) 11 (1–13)* 4 (1–12) 5.5 (1–9) Maternal BNP levels before 13.7 14.0 13.0 13.3 treatment, pg/ml (2.0–294.2) (2.0–294.2) (8.7–22.6) (2.0–96.1) Maximum maternal BNP levels 28.6 35.7 18.3 30.8 during treatment, pg/l (6.0–141.1) (11.9–118.0) (14.6–26.7) (6.5–141 .1 ) Delivery mode Vaginal delivery 27 9 3 15 Elective cesarean delivery 11 5 0 6 Urgent cesarean delivery 11 3 1 7 Urgent cesarean delivery 3 1 0 2 because of tachyarrhythmia Gestational age at birth, weeks 37 (28–40) 37 (34–39) 37 (36–38) 37 (28–40) Pre-term birth 10 (20.4) 3 (17.7) 1 (25.0) 6 (21.4) Birth weight, g 2,828 2,828 2,665 2,851 (1,828– (2,050– (2,506– (1,828– 3,808) 3,808) 3,508) 3,518) SGA <10th percentile 3 (6.1) 2 (11.7) 0 (0.0) 1 (3.6) Male 38 (77.6) 12 (70.6) 3 (75.0) 23 (82.1) Fetal hydrops at birth 3 (6.4) 0 (0.0) 1 (25.0) 2 (7.4) Neonatal tachyarrhythmia 15 (31.9) 8 (50.0) 2 (50.0) 5 (18.5) Antiarrhythmic medical 13 (27.7) 8 (50.0)* 2 (50.0) 3 (11.1) therapy after birth Fetal death 2 (4.1) 1 (5.9) 0 (0.0) 1 (3.6) Neonatal death within 1 month 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) Apgar score at 5 min 9 (0–10) 9 (0–10) 8.5 (6–9) 9 (5–10) Umbilical artery pH 7.31 7.32 7.31 7.30 (7.13–7.44) (7.22–7.37) (7.13–7.37) (7.21–7.44) Values are n, n (%), or median (range). *Significant difference when compared with fetuses with AFL (p < 0.05, the Steel-Dwass test). BNP ¼ brain natriuretic peptide; SGA ¼ small for gestational age; other abbreviations as in Table 1. most of these operations were performed for maternal or obstetrical indications such as previous cesarean delivery, arrest of labor, and infection; only 3 (6.1%; 95% CI: 1.3% to 16.9%) cesarean sec- tions were performed for fetal tachyarrhythmia. Recurrence of tachyarrhythmia was observed in 15 of 47 neonates (31.9%). Only 2 neonates continued to receive prophylactic digoxin after birth, and 1 did not have recurrence of tachyarrhythmia. Interest- ingly, 13 of 15 had had well-controlled tachyar- rhythmia before birth, but they still experienced recurrence postnatally. Except for 2 neonates with AFL who converted to sinus rhythm with electrical cardiove r sion, 13 neonate s require d antiarrhythmic treatment. Recurrence of tachyarrhythmia was observed within 2 weeks after birth in all neonates exce pt 1 with SVT in the third week. Notably, 10 of 15 had recu rr e nc e of tachya rr hy thm ia in the first 3 days. Intraventricular hemorrhage and periven- tricula r leuko ma la cia were detecte d in 1 (2.1%; 95% CI: 0.1% to 11.3%) and 4 (8.5% ; 95% CI: 2.4% to 20.4%) neonates after birth, respectively. There were no neonatal deaths. The same analysis was repeatedly conducted for the primary endpoint on the per-protocol set. After excluding 3 patients with life-threatening fetal mal- formations (tuberous sclerosis with cardiac tumors, suspected Costello syndrome with hypoplastic lungs, and heterotaxy syndrome) that were confirmed as violations of the exclusion criteria at data review committee, resolution of fetal tachyarrhythmia was obser ve d in 43 of 46 patien ts (93.5%; 95% CI: 82.1% to 98.6%). On the basis of echocardiographic assessment, 49 patients were classified into 3 groups: short VA SVT (n ¼ 17), long VA SVT (n ¼ 4), and AFL (n ¼ 28) (Table 1). Multiple arrhythmias were found in 4 fe- tuses; 3 fetuses with AFL had occasional short VA SVT, and 1 fetus with long VA SVT had occasional AFL. Gestational age at diagnosis was lower in pa- tients with short VA SVT compared with other ar- rhythmias. Primary and secondary outcomes did not vary by type of fetal tachyarrhythmia (Table 2). Recurrence of neonatal tachyarrhythmia was more comm on in patien ts with SVT than AFL (50.0% vs. 18.5%; p ¼ 0.03). In patients with short VA SVT and no hydrops, the resolution rate was 46.7% (7 of 15) with digoxin alone, 71.4% (5 of 7) with digoxin plus sotalol, and 100.0% (1 of 1) with digoxin in combination with flecainide, thereby resulting in a total resolution rate of 86.7% (Figure 2A). Five neonates had atrioventric- ular (AV) re-entrant tachycardia (AVRT), 2 had ectopic atrial tachycardia (EAT), and 1 had ventricular tachycardia all found after birth. In all, 4 patients with long VA SVT, including 1 patient with fetal hydrops, fetal tachyarrhythmia resolved (Figure 2B). In 1 neonate each, AVRT and EAT were found after birth. In patients with AFL without fetal hydrops, the resolution rate was 59.3% (16 of 27) with digoxin alone, 72.7% (8 of 11) with digoxin and sotalo l, and 50.0% (1 of 2) with digoxin and flecainide, resulting in an overall resolution rate of 92.6% (Figure 2C). In 1 neonate with AVRT, 1 with EAT, and 3 with AFL, the tachyarrhythmias were found after birth. The 2 neo- nates with AVRT and EAT had occasional short VA SVT in utero.
- 6. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 879 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 879 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 S A FE T Y O U TCO M E S. Maternal, fetal, and neonatal AEs related to the antiarrhythmic agents are shown in Table 3. Although maternal AEs related to trans- placental treatment were observed in 39 patients (78.0%), there was only 1 serious event: Mobitz type II AV block was observed but resolved immediately af- ter temporary discontinuation of digoxin and sotalol. Nausea or vomiting, the most common maternal adverse symptom, was observed in 27 patients (54.0%). Electrocardiographic abnormalities were detected in 19 patients (38.0%). Elevated brain natriuretic peptide concentrations were found in 25 patients (50.0%). Despite a relatively high incidence of maternal AEs, dose reduction allowed for contin- uatio n of transp lac e ntal treatment. Fetal AEs related to transplacental treatment were observed in 12 fetuses (24.0%). Serious AEs resulting in discontinuation of the protocol-treatment occurred in 4 fetuses. Fetal death occurred in 2 of 49 fetuses overall (4.1%; 95% CI: 0.5% to 14.0%). In 1 fetus heavy for gestational age (>5.0 SD), AFL developed with ascite s, cardia c effusion, and polyhyd ra mnio s at 26 weeks of gestation. After digoxin and sotalol combination therapy, the frequency and ventricular rate of fetal AFL decreased, but hydrops progressed, resulting in fetal death at 27 weeks of gestation. Post- mortem examination showed hypoplastic lungs, small ears, and flexion of the long finger in both hands, findings suggesting Costello syndrome. Another fetus of 34 weeks of gestation with a diag- nosis of short VA SVT once achieved sinus rhythm and resolved pleural effusion and ascites after digoxin and sotalol, but the tachyarrhythmia recurred at 36 weeks of gestation. SVT was sustained even after increased dosage of sotalol to 240 mg/day, and the fetus developed pleural effusion and ascites. The fetus died at 37 weeks of gestation during prepara- tions for cesarean section. These fetal deaths were mainly caused by progression of fetal heart failure secondary to AFL and SVT. In 1 fetus with AFL, 7:1 AV block was observed after starting the combination of digoxin and sotalol. Because the ventricular rate decreased to 50 beats/min for 5 min at 36 weeks of gestation, cesarean section was performed, and the newborn was treated by electrical cardioversion. In another fetus with AFL, 1:1 AV conduction at 275 beats/min was observed 5 days after starting the combination of digoxin and flecainide. The fetus progressed to ascites and pleural effusion and was delivered by cesarean section at 32 weeks of gesta- tion. AFL resolve d sponta ne ou sly just afte r birth. Neonatal AEs related to transplacental treatment were observed in 5 of 47 neonates (10.6%). Two of these AEs were serio us. Maternal serum digoxin concentrations after rapid initial saturation were not statistically different be- tween oral administration and intravenous injection (Online Table 2). Maternal and umbilical vein serum concentrations of the antiarrhythmic agents at de- livery are shown in Table 4. Interestingly, 7 of 13 had higher serum sotalol levels of umbilical vein than those of matern al vein. DISCUSSION The results of our study demonstrated that protocol- defined transplacental treatment for fetal SVT and AFL was effective and tolerable in 90% of cases (Central Illustration). However, it should be kept in mind that serious AEs may take place in fetuses and that tachyarrhythmia may recur within 2 weeks after birth. To the best of our knowledge, this is the first multicenter and largest prospective study of the safety and efficacy of protocol-defined transplacental treat- ment for fetal SVT and AFL. Dozens of studies showing the efficacy of fetal treatment have been published, but they included stated limitations related to retro- spective data collection and different protocols across centers. Two previous prospective studies had limi- tations related to the single-center design with small sample size (<20 cases) (11,12). In this study, digoxin was selected as the first-line agent (9) because of its relatively safe profile, long history of use during pregnancy, and clinician familiarity with its use (13– 15). Sotalol and flecainide were used as second-line and third-line agents, respectively, for cases with short VA SVT and AFL without fetal hydrops in this protocol (9). Compared with the previous studies, our multicenter prospective study demonstrated suffi- cient safety and efficacy. Some studies recommended sotalol or flecainide as primary therapy for fetal SVT and AFL (7,14–19). Two systematic reviews showed the superiority of flecainide as first-line treatment for fetal SVT (20,21). However, both studies com- mented on the lack of prospective studies as a limita- tion. Our protocol, which is based on the multicenter prospective study, can become baseline data for further prospective trials to establish the safest and most effe ctive treatm e nt for fetal tachy a rrh yth mia. Favorable efficacy of our protocol treatment was obtained with each type of fetal tachyarrhythmia. In this study, the measurement of AV and VA intervals with Doppler echocardiography was used to classify tachyarrhythmias (12,22,23). Short VA SVT is the typical pattern in re-entry tachycardia. Fetuses with short VA SVT and no hydr op s had a resolutio n rate of 47% with digoxin alone as the first-line drug and an
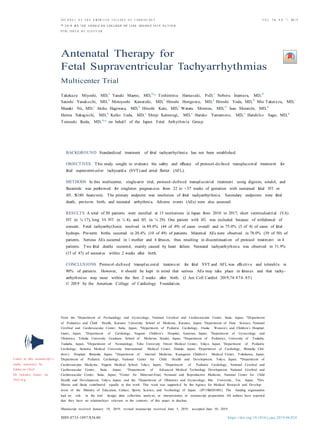
- 7. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 880 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 880 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 F IGUR E 2 Outcomes by Type of Fetal Tachyarrhy thm ia A Short VA SVT (n = 17) Non-hydrops Fetal hydrops Digoxin (n = 15) Digoxin & Sotalol (n = 2) Effective Ineffective Ineffective Effective n = 7 Digoxin & n = 1 Digoxin & n = 1 AVRT (2), VT (1) Sotalol (n = 7) EAT (1) Flecainide (n = 1) Effective Ineffective Effective n = 5 AVRT (2) Digoxin & Flecainide (n = 1) n = 1 Fetal death n = 1 EAT (1) Effective n = 1 AVRT (1) B Long VA SVT (n = 4) Non-hydrops Sotalol (n = 3) Fetal hydrops Sotalol (n = 1) Effective Effective n = 3 (Heterotaxy syndrome) EAT (1) n = 1 (Cardiac tumors) AVRT (1) (A) In fetuses with short ventriculoa tr ia l (VA) supraventricular tachycardia (SVT) and no hydrops, the resolution rate was 46.7% (7 of 15) with digoxin alone, 71.4% (5 of 7) with digoxin plus sotalol, and 100.0% (1 of 1) with digoxin plus flecainide, resulting in an overall resolution rate of 86.7%. Protocol treatment was discontinue d in 1 patient because of fetal death. Five cases of atrioventr ic ular re-entrant tachycardia (AVRT), 2 of ectopic atrial tachycardia (EAT), and 1 of ventricular tachycardia (VT) were found after birth. (B) In all 4 fetuses with long ventriculoatr ial supraventricular tachycardia, including 1 fetus with hydrops, fetal tachyarrhythmia resolved. One case each of atrioven- tricular re-entrant tachycardia and ectopic atrial tachycardia was observed after birth. (C) In atrial flutter (AFL) without fetal hydrops, the resolution rate was 59.3% (16 of 27) with digoxin alone, 72.7% (8 of 11) with digoxin plus sotalol, and 50.0% (1 of 2) with digoxin plus flecainide, resulting in an overall resolution rate of 92.6%. Protocol treatment was discontinued in 3 patients because of fetal serious adverse event (SAE) and death. One case of atrioventr icular re-entrant tachycardia, 1 of ectopic atrial tachycardia, and 3 of atrial flutter were found after birth. Neonatal tachyarrhythmia s are shown in the bottom of each box. Continued on the next page
- 8. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 881 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 881 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 F IGUR E 2 Continue d C AFL (n = 28) Non-hydrops Fetal hydrops Digoxin (n = 27) Digoxin & Sotalol (n = 1) Effective Ineffective Ineffective n = 16 AVRT (1), EAT (1) Effective Digoxin & Sotalol (n = 11) Ineffective n = 1 Progression of fetal hydrops AFL (1) n = 8 Digoxin & Flecainide n = 1 Fetal death AFL (2) (n = 2) (Suspected Costello syndrome) Effective Ineffective n = 1 n = 1 Discontinuation due to fetal SAE overall resolution rate of 87%, comparable to that of a previous review article (3). Both cases of short VA SVT and fetal hydrops achieved resolution in utero. Long VA SVT is a rare tachyarrhythmia suggesting EAT or atypical AVRT. Because digoxin was reported to be ineffective in long VA SVT (24), in this study protocol, sotalol and flecainide were used as first-line and second-line therapy, respectively. All 4 cases with long VA SVT including 1 with fetal hydrops had res- olution of fetal tachyarrhythmia. Therefore, our findings indicate the effectiveness of protocol treat- ment according to the waveforms assessed by Doppler echocardiography. Because no single agent is universally effective (12,15), it is important to give the most efficient drug at the lowest effective dose to avoid the risk of maternal and fetal morbidity. We believe that appropriate drug selection for each type of tachyarrhythmia contributes to avoiding maternal and fetal AEs. In this study, fetuses with AFL and no hydrops had a resolution rate of 59% with digoxin alone as first-line therap y and an overa ll resolutio n rate of 93%. Also in this study, AFL accounted for 60% of fetuses, a higher percentage than in previous reports (25% to 30%) (1,3,6). A large multicenter retrospective study showed that cardioversion at 5 and 10 days occurred in only 25% and 41% of fetuses with treated AFL, respectively (15). Sotalol was reported to effect a highe r propo rtion of fetal AFL termina tion than digoxin or fleca inide (15). A revie w article showed a fetal AFL resolution rate of 45% with digoxin alone, a findin g sugge stin g that if AFL persists, postnatal conve rsio n to sinus rhyth m may be prefe r re d over secon d-lin e trans pla ce nta l treatm e nt (3). However, our results showe d a high resolution rate in fetuses with AFL but no hydro p s, thus sugge sting that pre- mature delive ry should be limite d to treatment- refr ac tory AFL with hydrops. Our prospective study demonstrated a relatively high incidence of maternal AEs related to antiar- rhythmic agents. Maternal AEs, including gastroin- testinal symptoms and electrocardiographic abnormalities, were observed in 78% of patients; however, most of these AEs were minor, and dose
- 9. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 882 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 882 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 TAB LE 3 Materna l, Fetal, and Neonatal Treatment- Re la ted AEs and Serious AEs Patients Patients With With AE Serious AE Maternal (n ¼ 50) Gastrointestinal Nausea 20 0 (0.0) (40.0)* Vomiting 10 (20.0)* 0 (0.0) Stomach ache 1 (2.0) 0 (0.0) Anorexia 1 (2.0) 0 (0.0) Diarrhea 1 (2.0) 0 (0.0) General Malaise 1 (2.0) 0 (0.0) Limb pain 1 (2.0) 0 (0.0) Nervous system Headache 2 (4.0) 0 (0.0) Head discomfort 1 (2.0) 0 (0.0) Altered sensation of taste 1 (2.0) 0 (0.0) Drowsiness 1 (2.0) 0 (0.0) Numbness 1 (2.0) 0 (0.0) Increased thirst 1 (2.0) 0 (0.0) Obstetric Pre-term delivery 3 (6.0) 0 (0.0) Threatened pre-mature labor 1 (2.0) 0 (0.0) Polyhydramnios 1 (2.0) 0 (0.0) Electrocardiographic abnormalities Sinus bradycardia <60 beats/min 17 (34.0) 0 (0.0) Second-degree AV block 9 (18.0) 1 (2.0)† PR prolongation $200 ms 4 (8.0) 0 (0.0) Pre-mature ventricular contractions 2 (4.0) 0 (0.0) Nonspecific ST-T changes 1 (2.0) 0 (0.0) QTc prolongation $450 ms 1 (2.0) 0 (0.0) Clinical laboratory abnormalities Increased brain natriuretic peptide 25 (50.0) 0 (0.0) levels Liver dysfunction 1 (2.0) 0 (0.0) Impaired glycemic control 1 (2.0) 0 (0.0) Anemia 1 (2.0) 0 (0.0) Fetal (n ¼ 50) Fetal death 2 (4.0) 2 (4.0)‡ Electrocardiographic abnormalities Bradycardia <100 beats/min 6 (12.0) 1 (2.0)§ De novo arrhythmia 2 (4.0)k 1 (2.0)k Pre-mature atrial contractions 1 (2.0) 0 (0.0) General Decreased fetal movement 1 (2.0) 0 (0.0) Mild deceleration 3 (6.0) 0 (0.0) TAB LE 4 Mater na l and Umbilical Vein Serum Concentra t ions of the Antiarr hy thm ic Agents at Delive ry Digoxin Sotalol Flecainide (n ¼ 26) (n ¼ 13) (n ¼ 2)* Maternal vein serum levels, 1.2 371.5 31.1/440.3 ng/ml (0.3–2.7) (18.3–2,000.7) Umbilical vein serum levels, 0.6 440.0 15.7/305.1 ng/ml (0–1.5) (60.4–1,263.8) Umbilical-to-mater nal 53.5 107.1 50.5/69.3 vein ratio, % (0–100) (47.2–371.6)† Values are median (range) unless otherwise indicated. Analyses were performed in cases with both maternal and umbilical vein blood available at delivery. Serum digoxin concentrations were measured by enzyme-multiplied immunoassay tech- nique. Serum sotalol and flecainide concentrations were measured by high- performance liquid chromatography. *Data in this column are the values in each of the 2 cases. †7 of 13 had higher serum sotalol levels of umbilical vein than those of maternal vein. TAB LE 3 Continued Patients Patient s With With AE Serious AE Neonatal (n ¼ 47) Periventricular leukomalacia 1 (2.1) 0 (0.0) Ileus 1 (2.1) 1 (2.1)¶ Bradycardia <100 beats/min 1 (2.1) 0 (0.0) Clinical laboratory abnormalities Hyperbilirubinemia 1 (2.1) 0 (0.0) Erythrocytosis 1 (2.1) 0 (0.0) Hypoglycemia 1 (2.1) 1 (2.1)¶ Values are n (%). The causal relationship between AEs and antiarrhythmic agents was determined by the Independent Safety Evaluation Committee. *Nausea or vomiting were found in 27 patients (54.0%). During nausea or vomiting, median maternal digoxin levels were 1.96 ng/ml (range 0.94 to 3.77 ng/ml). †Mobitztype II AV block during the administration of digoxin (0.75 mg/day; 2.10 ng/ml) plus sotalol (160 mg/day). ‡In 1 fetus with AFL, 3 days after starting sotalol (160 mg/ day) in combination with digoxin (0.75 mg/day; 1.30 ng/ml), frequency and ven- tricular rate of fetal AFL decreased but hydrops progressed, resulting in fetal death at 27 weeks of gestation. In another fetus with short VA SVT, 2 days after increasing sotalol (240 mg/day) in combination with digoxin (0.375 mg/day; 1.55 ng/ml), fetal death was detected during preparation for cesarean section at 37 weeks of gestation. §In 1 fetus with AFL, fetal ventricular rate decreased to 50 beats/min for 5 min because of advanced AV block after starting the combination therapy of digoxin (0.50 mg/day; 2.45 ng/ml) plus sotalol (160 mg/day). kIn 1 fetus with short VA SVT, paroxysmal atrial fibrillation was observed 4 days after starting digoxin (0.75 mg/day; 0.90 ng/ml). In another fetus with AFL, 1:1 AV conduction at 275 beats/min was observed 5 days after starting the third-line combination therapy of digoxin (0.375 mg/day; 1.68 ng/ml) plus flecainide (200 mg/day; 425.8 ng/ml). ¶In 1 fetus with AFL, tachyarrhythmia was well controlled in utero by digoxin (0.25 mg/day; 1.36 ng/ml) and did not recur; however, ileus was observed 2 weeks after birth. In another fetus with short VA SVT, tachyarrhythmia was well controlled in utero by sotalol (160 mg/day); however, ectopic atrial tachycardia and hypoglycemia (31 mg/ml) were observed in the first day. AE ¼ adverse event; AV ¼ atrioventricular; other abbreviations as in Table 1. flecainide, or 10% with sotalol, and visual distur- bances occurred in 14% with flecainide) (15). Our re- sults suggest that most previous retrospective studies underestimated the incidence of maternal AEs. Combination therapy presents a greater risk of maternal and fetal AEs than monotherapy (8). Although serious maternal AEs were rare, occurrin g at rates similar to those in reporte d serie s (15,25), we Continued in the next column reduction allowed for continued protocol treatment. There are very few reports focusing on AEs related to transplacental antiarrhythmic treatment. Nausea, fa- tigue, and loss of appetite are well-known maternal AEs related to digoxin (8). Sinus bradycardia and AV block are common AEs with antiarrhythmic drugs (8). A previous report showed that one-third of mothers had likely drug-related AEs (e.g., nausea and dizzi- ness occurred in 38% with digoxin, 20% with
- 10. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 883 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 883 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 Short ventriculoatrial (VA) SVT or AFL (n = 45) ydrops Fetal H Digoxin: Maternal serum concentrations from 1.5 to 2.0 ng/mL Sotalol: Initial dose, 160 mg/day; Maximum dose, 320 mg/day Flecainide: Initial dose, 200 mg/day; Maximum dose, 300 mg/day CENT RAL IL LUS T RAT I O N Result s of the Transplacental Treat ment Protocol for Fetal Tachyarrhythmias Sustained fetal supraventricular tachycardia (SVT) or atrial flutter (AFL) ≥180 beats/min Singleton with 22 to <37 weeks of gestation (n = 49) Long VA SVT (n = 4) Non-h ydrops First-Choice Therapy Digoxin 54.8% (23/42) First-Choice Therapy Digoxin & Sotalol 33.3% (1/3) First-Choice Therapy Sotalol 100% (4/4) Second-Choice Therapy Digoxin & Sotalol 72.2% (13/18) Second-Choice Therapy Digoxin & Flecainide 100% (1/1) Second-Choice Therapy Flecainide Third-Choice Therapy Digoxin & Flecainide 66.7% (2/3) Antiarrhythmic Agents Miyoshi, T. et al. J Am Coll Cardiol. 2019;74(7):874–85. Antiarrhythmic agents were selected by types of fetal tachyarrhythm ia and/or presence of fetal hydrops. In short ventriculoatr ia l supra- ventricular tachycardia and atrial flutter without fetal hydrops, the resolution rate was 54.8% (23 of 42) with digoxin alone, 72.2% (13 of 18) with digoxin plus sotalol, and 66.7% (2 of 3) with digoxin plus flecainide, resulting in an overall resolution rate of 90.5% (38 of 42). In short ventriculoatr ia l supraventricular tachycardia and atrial flutter with fetal hydrops, the resolution rate was 33.3% (1 of 3) with digoxin plus sotalol and 100% (1 of 1) with digoxin plus flecainide, resulting in an overall resolution rate of 66.7% (2 of 3). In all 4 fetuses with long ventriculoatr ial supraventricular tachycardia, including 1 fetus with hydrops, fetal tachyarrhythmia resolved by sotalol alone. speculated about the need for serial drug concentra- tion monitoring and maternal electrocardiography to assess drug effects and toxicity, especially during dose escalation. Two fetal deaths occurred during combination therapy with digoxin and sotalol. In fetuses with hydrop s and SVT or AFL, arrhythmia-related mortality increased to 15% to 40%, compared with 0% to 4% in fetuses without hydrops (3–5,26–29). One fetal demise occurred 2 days after sotalol dose esca- lation. A previous study investigated the timing of 4 fetal deaths (3 SVT and 1 AFL). Three deaths occurred just days after the initiation of sotalol, and 1 death occurred after a dose increase (7). Several reports
- 11. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 884 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 884 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 showed fetal deaths within 3 days of transplacental flecainide treatment (28,29). It is difficult to draw conclusions about a potential AE of sotalol and fle- cainide in this group of fetuses at increased risk of prenatal demise. The occurrence of fetal death raises the question whether these agents have a proar- rhythmic effect because serum sotalol concentrations of umbilical vein can reach higher than those of maternal vein (11). In this regard, fetal magneto- cardiography has a potential role for detection of repolarization abnormalities or conduction defects that may lead to fetal sudde n death. ST U DY ST R E N G TH S. First of all, this was the first multicenter and largest prospective trial to confirm the safety and efficacy of protocol-defined trans- placental treatment for fetal SVT and AFL. Further- more, our results showed a high resolution rate even in fetuses with AFL, a treatment-refractory type of fetal tachyarrhythmia. Second, our findings indicate the effectiveness of protocol treatment. Notably, all 4 patients with long VA SVT were effectively treated with sotalol alone and with no mortality. Appropriate drug selection for each type of tachyarrhythmia is important not only to improve fetal and neonatal outcomes but also to avoid maternal and fetal AEs. Third, we prospectively confirmed accurate incidence of maternal, fetal, and neonatal AEs related to study antiarrhythmic agents. Our results showed a rela- tively high incidence of maternal AEs, thus suggest- ing underestimation in previous retrospective studies. Notably, serious AEs resulting in discontin- uation of the protocol treatment were found in 4 fe- tuses during combination therapy. This information will help obstetricians and pediatric cardiologists administering transplacental treatment for fetal SVT and AFL. ST U DY L IMITA TIO N S. First, this was a single-arm trial; however, this was the most completable pro- spective study design in the limited number of the cases in each year by referring the results of our retrospective survey and historical control data from the literature. Second, as a result of the limited sample size, only 4 patients with fetal hydrops and only 4 patients with long VA SVT were enrolled in this study. We used a strict definition of fetal hydrops (10) because we intended to limit combination therapy in truly severe cases in patients with fetal hydrops to avoid AEs to mothers and fetuses. Hence, our study did not have enough patients to make conclusions about combination therapy for the cases with fetal hydrops and about the therapy for long VA SVT. Third, beca use we used a treatm e nt protoc ol with 3 antiar rh ythm ic agents, it is diffic ult to analyze the safety and efficacy of each agent separately. However, the results of our first multicenter and largest prospective study could provide important baseline data as protocol-defined transplacental treatment for analyzing the effectiveness of future protocols, at least for fetal short VA SVT and AFL witho ut fetal hydrop s. CO NCLUSIONS Our study demonstrated that protocol-defined trans- placental treatment for fetal SVT and AFL was effec- tive and tolerable in 90% of cases. Maternal AEs were observed in 78% of patients; however, most AEs were minor, and dose reduction allowed for continued protocol treatment. However, it should be kept in mind that serious AEs may take place in fetuses and that tachyarrhythmia may recur within 2 weeks after birth even if it is well controlled in utero. We believe that our results will help optimize the design of future randomized controlled trials to establish the safest and most effective treatment for fetal tachy a rrh yth mia. A CK N OW L E D G ME N TS The authors thank Dr. Makoto Nishibatake (chairperson), Dr. Masao Nakagawa, Dr. Ichiro Kawabata, and Dr. Naokata Sumitomo for their contribution as members of the Independent Safety Evaluation Committee in this trial. The authors also thank Dr. Takeshi Kotake for measuring serum sotalol and fleca inid e concentrations. A D D RE SS F O R CO RRE SP O N D E N CE : Dr. Yasuki Maeno, Department of Pediatrics and Child Health, Kurume University School of Medicine, 67 Asahi-machi, Kurume 830-0011, Japan. E-mail: yasukim@med. kurume-u. a c.jp. Twitter: @YMaeno2. PERSPECTIVES COMPETENCY IN PATIENT CARE AND PROCE- DURAL SKILLS: Transplacental administration of digoxin, sotalol, or flecainide in singleton pregnancies from 22 to 37 weeks of gestation with sustained fetal SVT or AFL at ventricular rates $180 beats/min was effective and tolerated in 90%. Maternal AEs were frequent and usually mild, but they required treat- ment discontinuation in 8%, and fetal loss occurred in 4%. TRANSLATIONAL OUTLOOK: Further studies are needed to establish the safest and most effective antenatal treatment regimens for fetal supraventric- ular tachyarrhythmias.
- 12. J AC C V O L . 7 4 , N O. 7 , 2 0 19 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias 885 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 885 Miyoshi et al. Transplacenta l Treatment for Fetal Tachyarrhythmias J A C C V O L . 7 4 , N O . 7 , 2 0 1 9 A U G U S T 2 0 , 2 0 1 9 : 8 7 4 – 8 5 R E F E R E N C E S 1. Vergani P, Mariani E, Ciriello E, et al. Fetal ar- rhythmias: natural history and management. Ul- trasound Med Biol 2005;31:1–6. 2. Naheed ZJ, Strasburger JF, Deal BJ, Benson DW Jr., Gidding SS. Fetal tachycardia: mechanisms and predictors of hydrops fetalis. J Am Coll Cardiol 1996;27:1736– 40. 3. Krapp M, Kohl T, Simpson JM, Sharland GK, Katalinic A, Gembruch U. Review of diagnosis, treatment, and outcome of fetal atrial flutter compared with supraventricular tachycardia. Heart 2003;89:913–7. 4. Cuneo BF, Strasburger JF. Management strat- egy for fetal tachycardia. Obstet Gynecol 2000; 96:575–81. 5. Simpson J. Fetal arrhythmias. In: Allan L, Hornberger L, Sharland G, editors. Textbook of Fetal Cardiology. Cambridge, United Kingdom: Greenwich Medical Media, 2000:423–37. 6. Ueda K,Maeno Y,Miyoshi T, et al., on behalf of Japan Fetal Arrhythmia Group. The impact of in- trauterine treatment on fetal tachycardia: a nationwide survey in Japan. J Matern Fetal Neonatal Med 2018;31:2605–10. 7. Oudijk MA, Michon MM, Kleinman CS, et al. Sotalol in the treatment of fetal dysrhythmias. Circulation 2000;101:2721– 6. 8. Donofrio MT, Moon-Grady AJ, Hornberger LK, et al., American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Council on Cardiovascular and Stroke Nursing. Diagnosis and treatment of fetal cardiac disease:a scientific statement from the American Heart As- sociation. Circulation 2014;129:2183–242. 9. Miyoshi T, Maeno Y, Sago H, et al., Japan Fetal Arrhythmia Group. Antenatal antiarrhythmic treatment for fetal tachyarrhythmias: a study protocol for a prospective multicentre trial. BMJ Open 2017;7:e016597. 10. Anandakumar C, Biswas A, Wong YC, et al. Management of non-immune hydrops: 8 years’ experience. Ultrasound Obstet Gynecol 1996;8: 196–200. 11. Oudijk MA, Ruskamp JM, Ververs FF, et al. Treatment of fetal tachycardia with sotalol: transplacental pharmacokinetics and pharmaco- dynamics. J Am Coll Cardiol 2003;42:765–70. 12. Fouron JC, Fournier A, Proulx F, et al. Man- agement of fetal tachyarrhythmia based on supe- rior vena cava/aorta Doppler flow recordings. Heart 2003;89:1211–6. 13. Jaeggi E, Fouron JC, Drblik SP. Fetal atrial flutter: diagnosis, clinical features, treatment, and outcome. J Pediatr 1998;132:335–9. 14. Krapp M, Baschat AA, Gembruch U, Geipel A, Germer U. Flecainide in the intrauterine treatment of fetal supraventricular tachycardia. Ultrasound Obstet Gynecol 2002;19:158–64. 15. Jaeggi ET, Carvalho JS, De Groot E, et al. Comparison of transplacental treatment of fetal supraventricular tachyarrhythmias with digoxin, flecainide, and sotalol: results of a nonrandomized multicenter study. Circulation 2011;124:1747–54. 16. Shah A, Moon-Grady A, Bhogal N, et al. Effectiveness of sotalol as first-line therapy for fetal supraventricular tachyarrhythmias. Am J Cardiol 2012;109:1614– 8. 17. Uzun O, Babaoglu K, Sinha A, Massias S, Beattie B. Rapid control of foetal supraventricular tachycardia with digoxin and flecainide combina- tion treatment. Cardiol Young 2012;22:372–80. 18. Sridharan S, Sullivan I, Tomek V, et al. Flecai- nide versus digoxin for fetal supraventricular tachycardia: comparison of two drug treatment protocols. Heart Rhythm 2016;13:1913–9. 19. Ekiz A, Kaya B, Bornaun H, et al. Flecainide as first-line treatment for fetal supraventricular tachycardia. J Matern Fetal Neonatal Med 2018;31: 407–12. 20. Alsaied T, Baskar S, Fares M, et al. First-line antiarrhythmic transplacental treatment for fetal tachyarrhythmia: a systematic review and meta- analysis. J Am Heart Assoc 2017;6:e007164. 21. Hill GD, Kovach JR, Saudek DE, Singh AK, Wehrheim K, Frommelt MA. Transplacental treatment of fetal tachycardia: a systematic re- view and meta-analysis. Prenat Diagn 2017;37: 1076–83. 22. D’Alto M, Russo MG, Paladini D, et al. The challenge of fetal dysrhythmias: echocardio- graphic diagnosis and clinical management. J Cardiovasc Med 2008;9:153– 60. 23. Jaeggi ET, Nii M. Fetal brady- and tachyar- rhythmias: new and accepted diagnostic and treatment methods. Semin Fetal Neonatal Med 2005;10:504–14. 24. Jaeggi E, Fouron JC, Fournier A, van Doesburg N, Drblik SP, Proulx F. Ventriculo-atrial time interval measured on M mode echocardiog- raphy: a determining element in diagnosis, treat- ment, and prognosis of fetal supraventricular tachycardia. Heart 1998;79:582–7. 25. Moatassim S, Touleimat S, Hazelzet T, et al. Maternal complications induced by digoxin treat- ment of fetal tachycardia: a retrospective series of 18 cases. J Gynecol Obstet Hum Reprod 2018;47: 35–8. 26. Lisowski LA, Verheijen PM, Benatar AA, et al. Atrial flutter in the perinatal age group: diagnosis, management and outcome. J Am Coll Cardiol 2000;35:771–7. 27. van Engelen AD, Weijtens O, Brenner JI, et al. Management outcome and follow-up of fetal tachycardia. J Am Coll Cardiol 1994;24:1371–5. 28. Simpson JM, Sharland GK. Fetal tachycardias: management and outcome of 127 consecutive cases. Heart 1998;79:576–81. 29. Allan LD, Chita SK, Sharland GK, Maxwell D, Priestley K. Flecainide in the treatment of fetal tachycardias. Br Heart J 1991;65:46–8. KE Y WO RD S a dve r se eve nt, atri al flutter , fetal e c hoca r diogr a phy , fetal ta c hy a r r hy thm ia , suprave ntricular tachycardi a, tra nspla ce nta l treatme nt A P P E N D I X For supplemental tables, please see the online version of this paper.