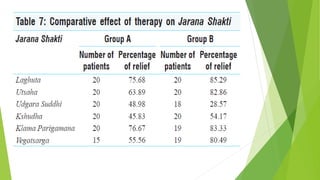
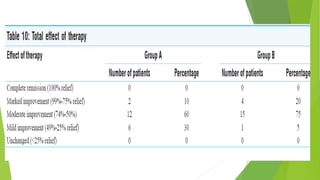
This document summarizes a study on the effect of eating one meal per day (Ekakala Bhojana) in patients with weak digestion (Agnimandya). The study found that eating one meal per day significantly improved patients' appetite and digestion over 10 days compared to those who received medicine. Specifically, eating one meal per day led to a 65.19% improvement in digestive capacity, compared to 55.76% for those receiving medicine. The study concludes that eating one meal per day is an effective dietary treatment for Agnimandya as recommended in classical Ayurvedic texts.