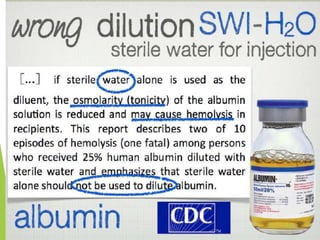
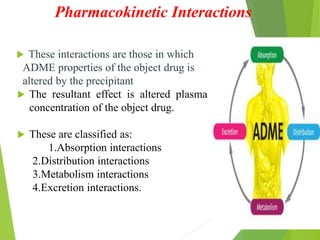
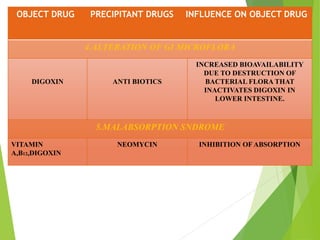
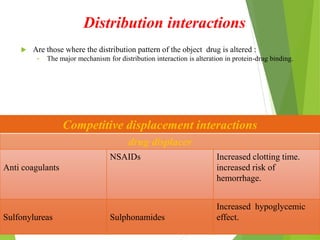
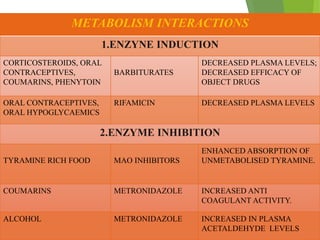
Drug interaction occurs when one drug alters the effects of another drug. It can happen through various mechanisms: pharmaceutical interactions when drugs physically interact; pharmacokinetic interactions which affect absorption, distribution, metabolism, or excretion of the drug; and pharmacodynamic interactions where drugs interact at the site of action. Factors like multiple drug use, diseases, age, and non-compliance can contribute to interactions. Careful evaluation of risks and close patient monitoring can help reduce harmful interactions.