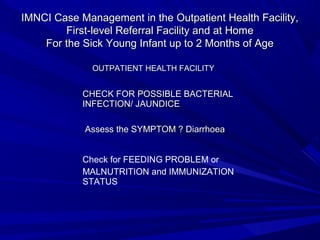
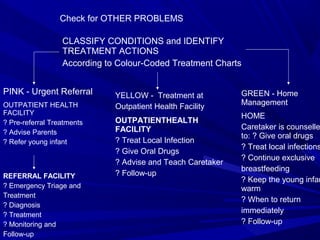
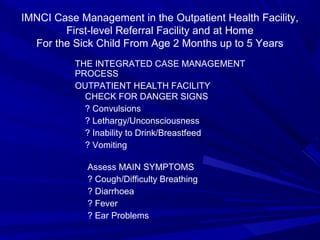
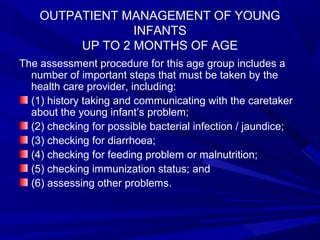
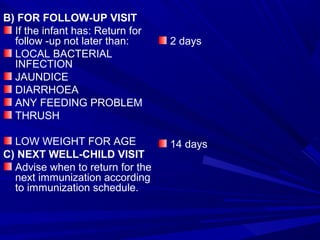
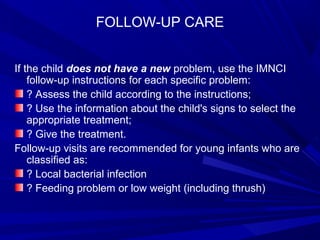
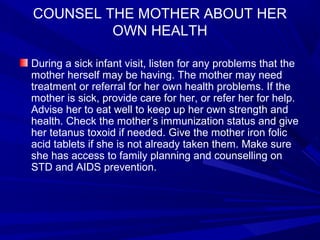
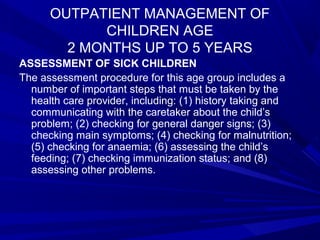
The document discusses the Integrated Management of Childhood Illnesses (IMNCI) strategy developed by WHO and UNICEF to provide integrated care for young infants and children for common childhood illnesses. The IMNCI strategy includes improving the case management skills of health staff, strengthening the overall health system, and improving family and community health care practices. It provides guidelines for assessing, classifying, treating and counseling caretakers of sick young infants and children based on their symptoms and condition.