General considerations
• Structuredapproach
• Call for help early
• Team leadership
• Situational awareness
• Non verbal skills
• Task management
• Decision making
3.
Structured approach
Plan fordealing with most of emergencies
• Four stages:
1. Identification of the emergency
2. Immediate actions
3. Specific treatment
4. Further management and follow up.
LA toxicity
Recognition
CNS:
• Suddenalteration in mental status
• Severe agitation or loss of consciousness
• Tonic- clonic convulsions
CVS:
• Sinus bradycardia
• Conduction blocks
• Asystole
• VF/VT
7.
Immediate Management
• Stopinjecting
• Call for help
• A: maintain airway and if necessary, secure it with a ETT.
• B: 100% oxygen and ensure adequate lung ventilation
• C: confirm or establish intravenous access.
• D: control seizures: give benzodiazepines, thiopental or propofol in
small increments, check glucose
8.
LA toxicity SpecificManagement
• In cardiac arrest start CPR and follow ACLS
• Treat: Hypotension, bradycardia and tachyarrhythmia
• Lipid Emulsion: initial intravenous bolus injection of 20% lipid
emulsion 1.5 ml/kg over 1 min and start an intravenous infusion of
20% lipid emulsion at 15ml/kg/h. After 5 min ( if still unstable) give a
maximum of two repeat boluses. Double the rate to 30 ml/kg/ hr at
any time after 5 min.
9.
LA Toxicity –Follow Up
• Transfer to HDU
• Serial amylase for two days, to exclude pancreatitis
• Report the case to the national database.
MH Recognition
• Unexplainedincrease in ETCO2+
• Unexplained tachycardia+
• Unexplained increase in oxygen requirement+
• Presence of muscle rigidity or Masseter spasm
• Temperature changes are late sign
12.
MH immediate management
•Stop all trigger agents
• Call for help
• A: maintain airway
• B: install clean breathing system and hyperventilate with 100% O2 high flow
• C: Cold IV fluids
• D: maintain anesthesia with IV agent
• E: Ice packs, bladder irrigation, NG irrigation
• Abandon/ finish surgery as soon as possible
• Muscle relaxation with non depolarizing NM blocking agent
13.
MH specific Management
Dantrolene
•Mechanism of action: dantrolene uncouples the excitation
contraction process by binding to the ryanodine receptor thereby
preventing the release of Ca2+ from the sarcoplasmic reticulum
striated muscles.
• Dose : 2.5 mg/kg immediate iv bolus. Repeat 1mg/kg bolus as
required to max 10mg/kg.
14.
MH follow up
•Transfer to HDU
• Monitor K and CK
• Monitor U and E’s AKI ( rhabdomyolysis )
• Risk of compartment syndrome
• Referral to local MH unit
• Family counselling
15.
High/ complete spinal
•Definition : clinical block well above the level required for surgical
anesthesia
• The term complete spinal imply anesthetic block involving the cervical
spine and above.
16.
Complete spinal recognition
cardiorespiratoryneurological
hypotension Nausea and anxiety
bradycardia Arm/ hand dysarthria or paralysis
Respiratory compromise High sensory level block
apnea Cranial nerve involvement
Reduced oxygen saturation Loss consciousness
Difficult speaking/ cough
Cardiac arrest
17.
Complete spinal management
•Supportive and dependent on the degree and height of the block
• ABCDE
feature management
Bradycardia Vagolytics.. Atropine
Sympathomimetics.. Ephedrine, adrenaline
Hypotension Vasopressors.. Metaraminol, phenylephrine,
fluid boluses
Respiratory dysfunction Oxygenation, intubation and ventilation
Loss of consciousness Secure airway supportive measures
18.
Complete spinal followup
• Sedation and mechanical ventilation needs to be continued until
there is clear evidence of adequate spontaneous respiratory function
• Hemodynamic changes should progressively improve as the block
resolves
• Post operative discussion with the patient
• If clinical suspicion of an anatomical abnormality - investigate
Recognition
• Temporal lobarherniation beneath tentorium cerebelli( uncal
herniation)- causes cranial nerve III palsy ( dilatation of pupils
followed by movement of eye down and out).
• Herniation of cerebellar peduncles through foramen magnum
(tonsillar herniation). Pressure on the brainstem causes the Cushing
reflex- hypertension, bradycardia and Cheyne stokes respiration.
• Subfalcine herniation occurs when the cingulate gyrus on the medial
aspect of the frontal lobe is displaced across the midline under the
free edge of the falx cerebri and may compress the the anterior
cerebral artery
21.
Medical management
ABCDE
• Ventilatewith 100% O2 ( PaO2> 13 Kpa)
• CO2 control ( 4.5 – 5 Kpa) moderate hyperventilation
• Ensure adequate MAP
• Position- ensure adequate venous drainage
• Increase sedation
• Temperature control
• Barbiturates
• Hyperosmolar therapy( Mannitol / hypertonic saline)
• Seizure control
22.
Surgical Management
• CSFdrainage- EVD
• Decompressive craniotomy
• Evacuation of hematoma
• Lobectomy/ removal of contusion
23.
Major obstetric hemorrhage
Definitions
•Primary postpartum hemorrhage is blood loss greater than 500 ml in
the 24 hours following delivery
• Minor PPh: 500- 1000 ml
• Moderate 1000 – 1500 mls
• Severe > 2000 mls
• Generally blood loss > 1500 mls and ongoing more than 150 ml per
minute accepted as MOH
24.
MOH causes
Four Ts
•Tone ( uterine atony 70% of cases)
• Tissue
• Trauma
• Thrombin
25.
MOH management
Key Points
•Communication
• Resuscitation/ replacement of fluid
• Arresting the bleeding
• Monitoring and investigation
26.
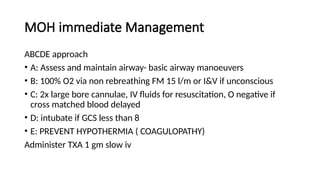
MOH immediate Management
ABCDEapproach
• A: Assess and maintain airway- basic airway manoeuvers
• B: 100% O2 via non rebreathing FM 15 l/m or I&V if unconscious
• C: 2x large bore cannulae, IV fluids for resuscitation, O negative if
cross matched blood delayed
• D: intubate if GCS less than 8
• E: PREVENT HYPOTHERMIA ( COAGULOPATHY)
Administer TXA 1 gm slow iv
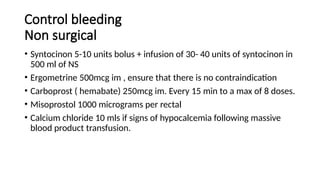
Control bleeding
Non surgical
•Syntocinon 5-10 units bolus + infusion of 30- 40 units of syntocinon in
500 ml of NS
• Ergometrine 500mcg im , ensure that there is no contraindication
• Carboprost ( hemabate) 250mcg im. Every 15 min to a max of 8 doses.
• Misoprostol 1000 micrograms per rectal
• Calcium chloride 10 mls if signs of hypocalcemia following massive
blood product transfusion.
29.
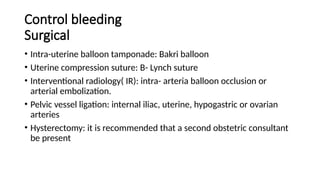
Control bleeding
Surgical
• Intra-uterineballoon tamponade: Bakri balloon
• Uterine compression suture: B- Lynch suture
• Interventional radiology( IR): intra- arteria balloon occlusion or
arterial embolization.
• Pelvic vessel ligation: internal iliac, uterine, hypogastric or ovarian
arteries
• Hysterectomy: it is recommended that a second obstetric consultant
be present
30.
Cardiac Tamponade
post cardiacintervention
Definition
• Rapid compression of the heart by accumulation of fluid( often blood)
within the pericardial sac that reduces ventricular filling and CO and is
a surgical emergency
• Obstructive shock
31.
Recognition
• Beck’s triad
Hypotension,elevated jvp and muffled heart sounds.
Although pathognomonic, these signs are collectively present in a small
number of patients presenting with cardiac tamponade.
• Pulsus paradoxus : an exaggerated fall in systemic arterial blood
pressure during the inspiratory phase of spontaneous ventilation.
• Kussmaul sign: paradoxical increase in cvp with inspiration
• Pulseless electric activity (PEA) cardiac arrest can follow
32.
Investigation
• Trans OesophagealEchocardiiography:
Gold standard for Dx. Presence of 1 cm pericardial separation
• TTE: more unreliable
• Cxr: widened mediastinum with globular heart shadow, difficult to
interpret
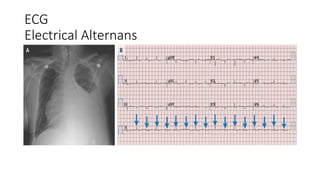
• ECG : pulsus alternans
Immediate management
ABCDE
• A:”if awake give O2 via non-rebreather facemask- 15 l/min
• B: ensure adequate oxygenation and ventilation. Minimize PEEP in
ventilated patients to ensure filling ( to avoid limiting venous return)
• C: Invasive Hemodynamic monitoring ( IABP, CVP) cross match blood.
Inotropic support , cautious fluid resuscitation
• Monitor GCS
• Reverse any coagulopathy
36.
Specific Management
• NeedlePericardiocentesis: ineffective as cannot remove clotd
• Resternotomy : usually the only option
• Pericardotomy: video assisted thoracoscopic approach is less invasive
creating drainage window between pleura and pericardium
37.
Resternotomy
• If stable-plan to transfer to theater
• Full invasive monitoring, inotropes and fluids are required.
• Senior anesthetist with cardiothoracic experience
• Induction on operation table after patient prepared and draped
• Induction:
Opiate: Fentanyl ( 2-10 mcg/kg)
Induction agent: thiopentne 1-4 mg/kg or Etomidate 0.1 – 0.2 mg/kg
Muscle relaxant : rocuronium 0.6- 1 mg/kg
• Hemodynamics may improve upon sternal opening and drainage of fluid
38.
Stridor in achild
• Definition
Harsh vibratory sound produced when airway becomes partially
obstructed, resulting in turbulent airflow in the respiratory passages
39.
Key points
• Multidisciplinaryteam approach- pediatrics, ENT, Theatre, and local
paeds intensive care
• Call for senior help early
• Avoid disturbing the child, crying and agitation may precipitate
complete airway obstruction.
• Avoid cannulation and x rays.
• Parents always present with child
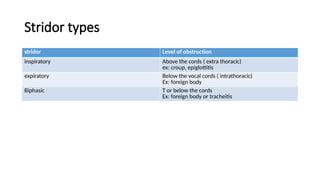
Stridor types
stridor Levelof obstruction
inspiratory Above the cords ( extra thoracic)
ex: croup, epiglottitis
expiratory Below the vocal cords ( intrathoracic)
Ex: foreign body
Biphasic T or below the cords
Ex: foreign body or tracheitis
42.
Initial management
ABCD
• Callfor help senior anesthetist and ENT staff,
• Administer high flow oxygen as tolerated, often by parent giving O2.
• Place sats probe on child
• Administer 4 mg/kg adrenaline nebulizer
• Move child to area suitable for inhalational induction
43.
Further management
• Preparationas for difficult airway, full equipments available and checked, 2nd
experienced anesthetist, experienced airway assistant present.
• Inhalational induction with 100% O2 and agent of choice usually sevoflurane. Child
remains in sitting position.
• IV access can be obtained at this point and 20 mcg/kg of atropine premedication
administered
• Child is laid flat before intubation
• Use smaller ETT than predicted, intubate and secure the airway
• Administer appropriate antibiotic therapy based on local guidelines after swab and
blood culture obtained
• Transfer to critical care environment for further management.
44.
Foreign body Aspiration
•Peak incidence at 1-2 years of age
• Partial obstruction of a lower airway may cause air trapping behind
the foreign body with pneumothorax, pneumomediastinum and
surgical emphysema
• Rigid bronchoscopy with the patient breathing spontaneously under
deep inhalational anesthesia supplemented with up to 3mg/kg of
topical lidocaine will confirm the diagnosis and allow for removal of
foreign body