
Download to read offline
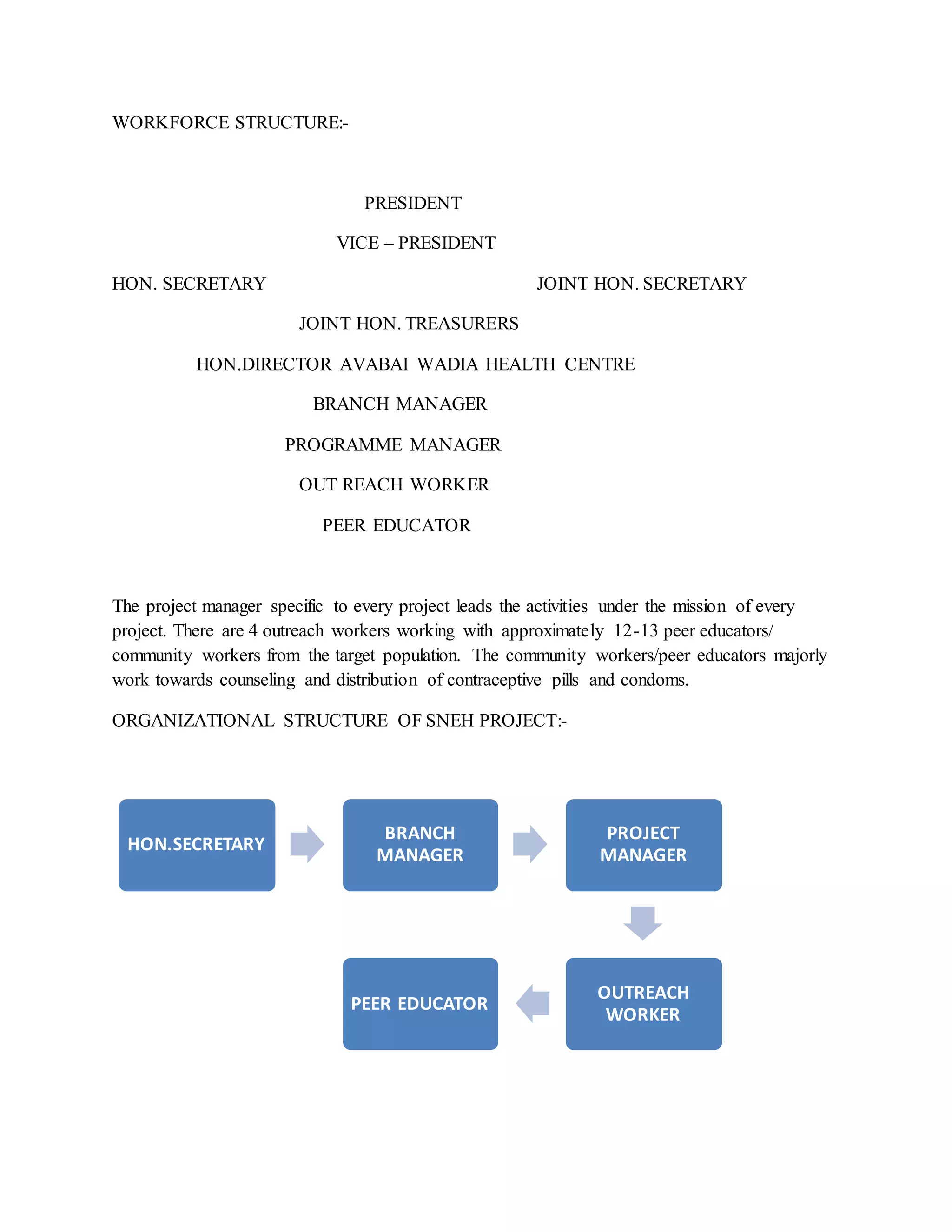
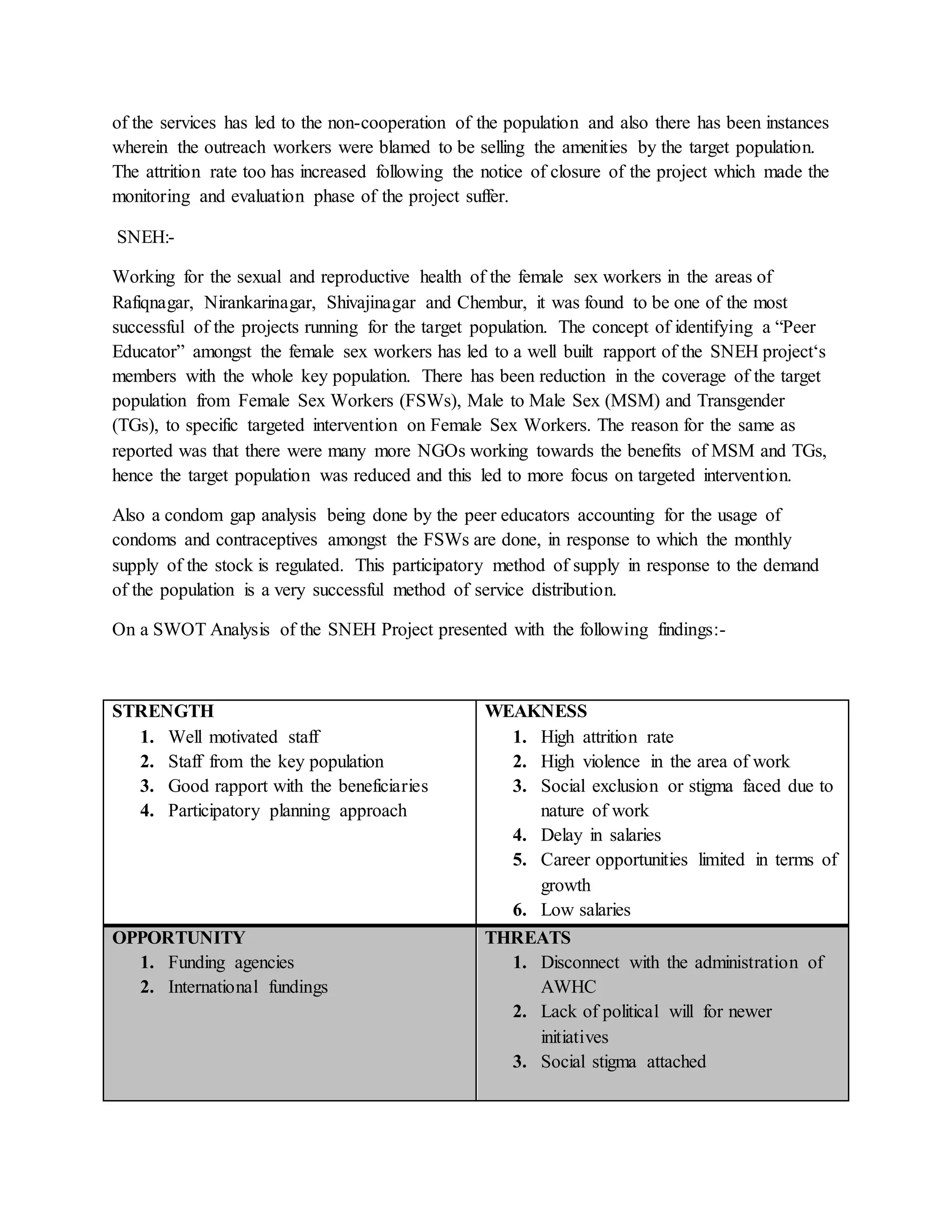
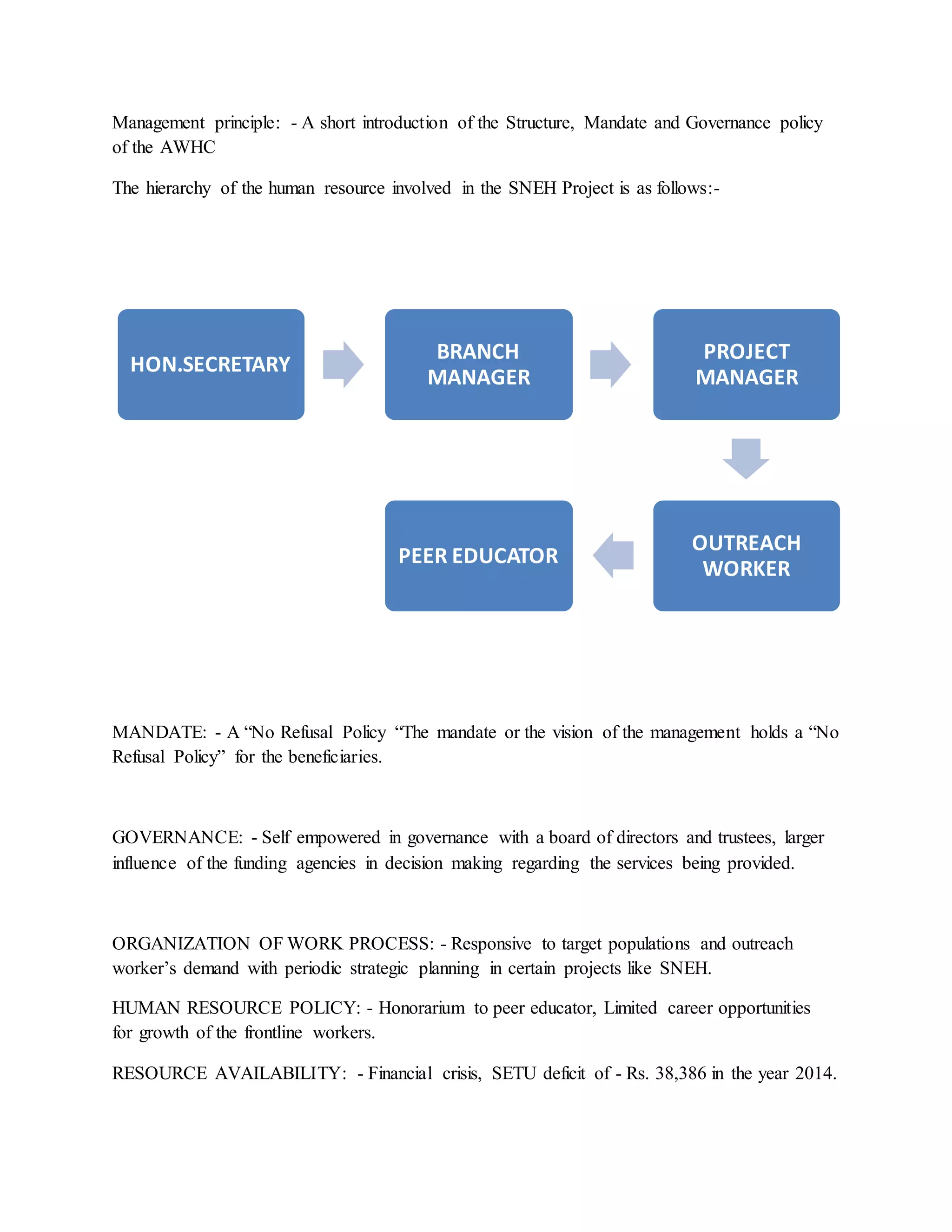
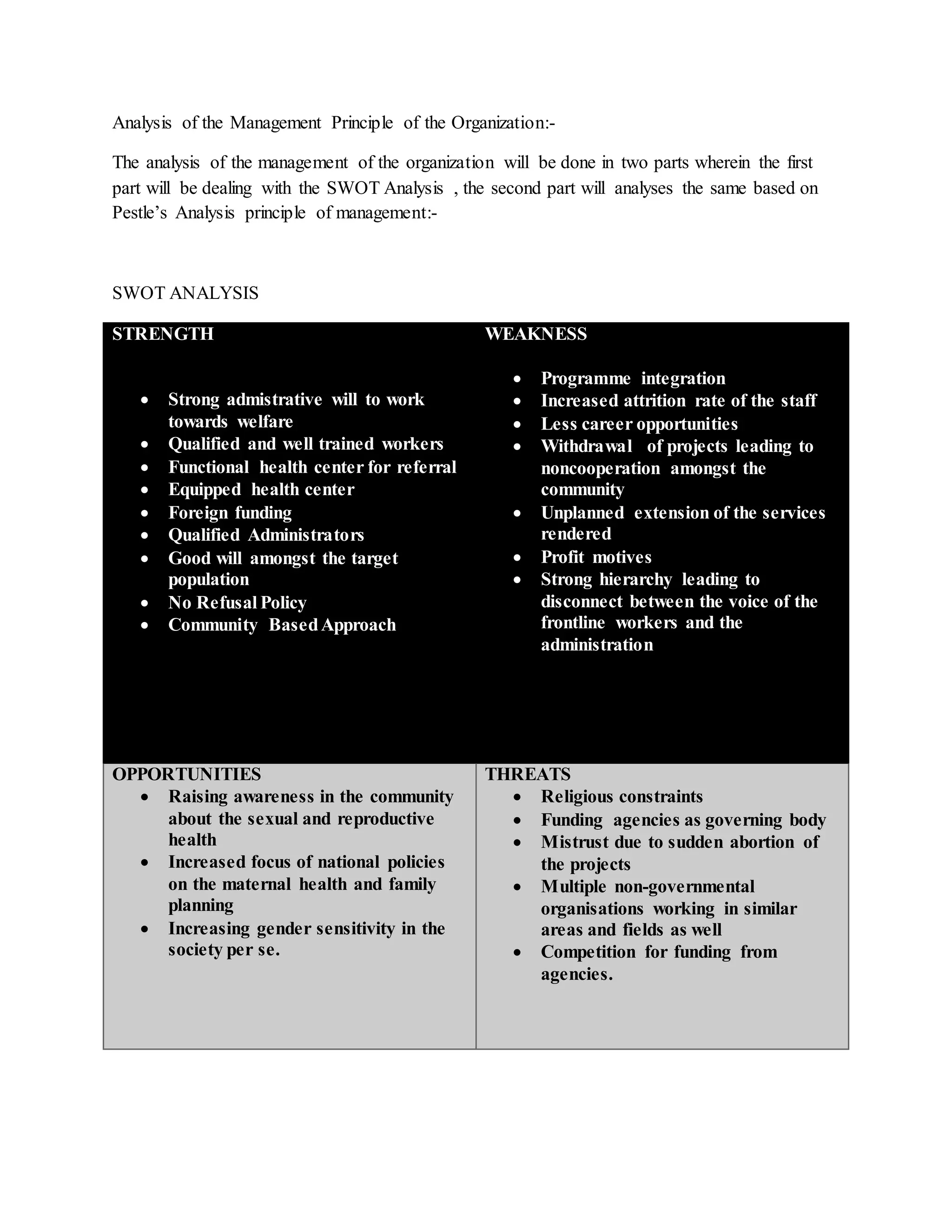

The document summarizes an internship report on an organization called Avabai Wadia Health Centre that provides sexual and reproductive health services. It describes the organization's mission, workforce structure, and services provided under various projects targeting different populations, such as female sex workers, migrants, and adolescents. The summary analyzes some of the organization's challenges, such as overreliance on funding that affects sustainability when projects end, and lack of community participation that impacts uptake of services. It also evaluates specific projects, finding the SNEH project for female sex workers to be most effective due to its participatory approach including peer educators from the target community.


































































![Countdown confreport web[1]](https://cdn.slidesharecdn.com/ss_thumbnails/countdownconfreportweb1-100810075655-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)