Interface dermatitis
Dr.Shanmathi Sethumadhavan, 2nd
year PG,
Dept of DVL , TVMCH
Moderator: Dr. P.Sivayadevi, Associate Professor
Indian Journal of Dermatology, Venereology, and Leprology | May-June 2013 | Vol 79 | Issue 3
4.
Introduction
• Primary pathologyinvolves the "interface“ –DEJ
• Components of the interface- single anatamico –physiological unit
Basal layer of epidermis
Dermoepidermal junction
Adventitial dermis –papillary + periadnexal dermis
• Cell mediated immunologic reactions whose targets are basal
keratinocytes that reside above the dermoepidermal junction
5.
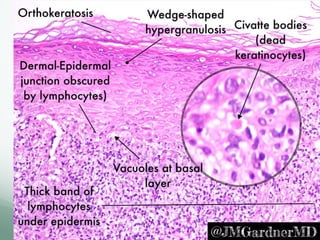
• Pattern ofinflammation in which lymphocytes aggregate around the
dermal-epidermal junction obscuring the junction at scanning
magnification.
• Vacuolar change , necrotic keratinocytes , spongiosis
• T-cell-mediated cytokine damage is most likely mechanism
• cytotoxic damage, or apoptosis of keratinocytes
• become detached from their neighbors,
• become round,
• undergo a sequence of events,
– degradation of nuclear DNA,
– lysis of nuclei
– coagulation of proteins in cytoplasm, without spilling enzymes
• Termed as dyskeratotic cells,
• When they find their way into papillary dermis, termed as
colloid, cytoid or Civatte bodies
6.
Morphological changes
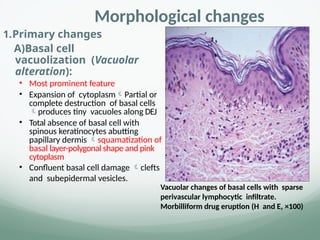
1.Primary changes
A)Basalcell
vacuolization (Vacuolar
alteration):
• Most prominent feature
• Expansion of cytoplasmPartial or
complete destruction of basal cells
produces tiny vacuoles along DEJ
• Total absence of basal cell with
spinous keratinocytes abutting
papillary dermis squamatization of
basal layer-polygonal shape and pink
cytoplasm
• Confluent basal cell damage clefts
and subepidermal vesicles.
Vacuolar changes of basal cells with sparse
perivascular lymphocytic infiltrate.
Morbilliform drug eruption (H and E, ×100)
7.
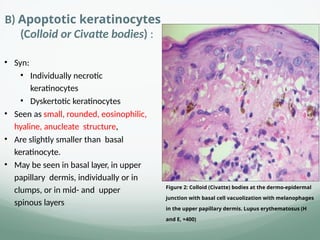
B) Apoptotic keratinocytes
(Colloidor Civatte bodies) :
• Syn:
• Individually necrotic
keratinocytes
• Dyskertotic keratinocytes
• Seen as small, rounded, eosinophilic,
hyaline, anucleate structure,
• Are slightly smaller than basal
keratinocyte.
• May be seen in basal layer, in upper
papillary dermis, individually or in
clumps, or in mid- and upper
spinous layers
Figure 2: Colloid (Civatte) bodies at the dermo‐epidermal
junction with basal cell vacuolization with melanophages
in the upper papillary dermis. Lupus erythematosus (H
and E, ×400)
9.
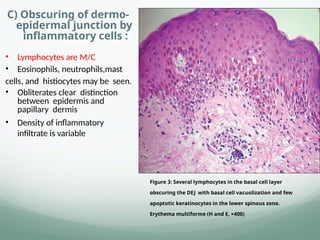
C) Obscuring ofdermo-
epidermal junction by
inflammatory cells :
• Lymphocytes are M/C
• Eosinophils, neutrophils,mast
cells, and histiocytes may be seen.
• Obliterates clear distinction
between epidermis and
papillary dermis
• Density of inflammatory
infiltrate is variable
Figure 3: Several lymphocytes in the basal cell layer
obscuring the DEJ with basal cell vacuolization and few
apoptotic keratinocytes in the lower spinous zone.
Erythema multiforme (H and E, ×400)
10.
2. Secondary changes
Epidermalchanges:
Depend on
disease
time of biopsy in course of evolution or devolution of disease
site of biopsy
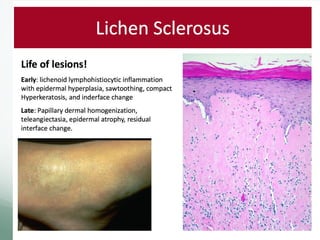
Acanthosis, hypergranulosis -LP
Thick compact orthokeratotic stratum corneum- LP
Thin and atrophic epidermis –LE , atrophic LP
Irregular epidermal hyperplasia- verrucous DLE
11.
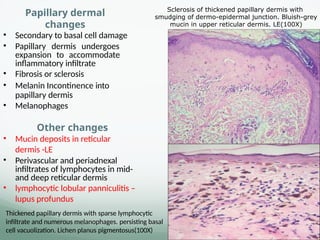
Papillary dermal
changes
• Secondaryto basal cell damage
• Papillary dermis undergoes
expansion to accommodate
inflammatory infiltrate
• Fibrosis or sclerosis
• Melanin Incontinence into
papillary dermis
• Melanophages
Other changes
• Mucin deposits in reticular
dermis -LE
• Perivascular and periadnexal
infiltrates of lymphocytes in mid-
and deep reticular dermis
• lymphocytic lobular panniculitis –
lupus profundus
Sclerosis of thickened papillary dermis with
smudging of dermo-epidermal junction. Bluish-grey
mucin in upper reticular dermis. LE(100X)
Thickened papillary dermis with sparse lymphocytic
infiltrate and numerous melanophages. persisting basal
cell vacuolization. Lichen planus pigmentosus(100X)
12.
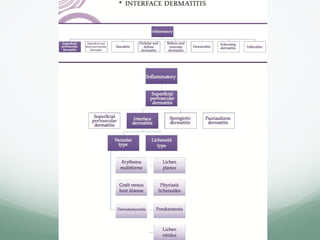
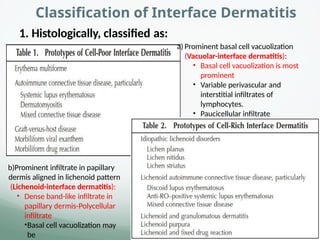
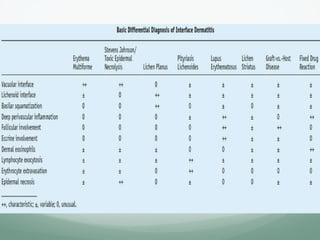
Classification of InterfaceDermatitis
b)Prominent infiltrate in papillary
dermis aligned in lichenoid pattern
(Lichenoid-interface dermatitis):
• Dense band-like infiltrate in
papillary dermis-Polycellular
infiltrate
•Basal cell vacuolization may
be
1. Histologically, classified as:
a) Prominent basal cell vacuolization
(Vacuolar-interface dermatitis):
• Basal cell vacuolization is most
prominent
• Variable perivascular and
interstitial infiltrates of
lymphocytes.
• Paucicellular infiltrate
13.
Parenthetically, atrue lichenoid infiltrate is
restricted to the papillary dermis
seen typically in interface dermatitis,
Band like infiltrate often extends into the reticular dermis without any interface
‐
changes
Granulomatous conditions
Tuberculosis verrucosa cutis (TBVC)
Lupus vulgaris
Benign, premalignant, and malignant conditions
Lichenoid keratosis
Paget’s disease (both mammary and extramammary)
Bowen’s disease
Resolving malignant melanoma
14.
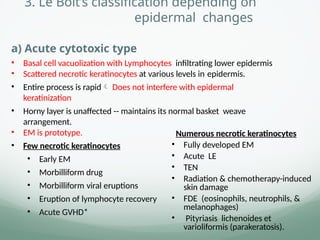
3. Le Boit’sclassification depending on
epidermal changes
a) Acute cytotoxic type
• Basal cell vacuolization with Lymphocytes infiltrating lower epidermis
• Scattered necrotic keratinocytes at various levels in epidermis.
• Entire process is rapid Does not interfere with epidermal
keratinization
• Horny layer is unaffected -- maintains its normal basket weave
arrangement.
• EM is prototype.
• Few necrotic keratinocytes
• Early EM
• Morbilliform drug
• Morbilliform viral eruptions
• Eruption of lymphocyte recovery
• Acute GVHD*
Numerous necrotic keratinocytes
• Fully developed EM
• Acute LE
• TEN
• Radiation & chemotherapy-induced
skin damage
• FDE (eosinophils, neutrophils, &
melanophages)
• Pityriasis lichenoides et
varioliformis (parakeratosis).
15.
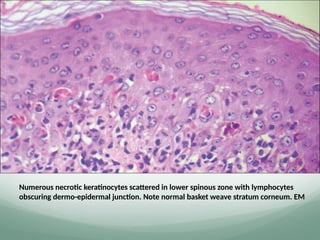
Numerous necrotic keratinocytesscattered in lower spinous zone with lymphocytes
obscuring dermo-epidermal junction. Note normal basket weave stratum corneum. EM
16.
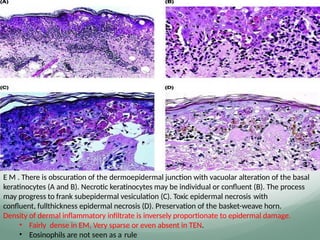
E M .There is obscuration of the dermoepidermal junction with vacuolar alteration of the basal
keratinocytes (A and B). Necrotic keratinocytes may be individual or confluent (B). The process
may progress to frank subepidermal vesiculation (C). Toxic epidermal necrosis with
confluent, fullthickness epidermal necrosis (D). Preservation of the basket-weave horn.
Density of dermal inflammatory infiltrate is inversely proportionate to epidermal damage.
• Fairly dense in EM, Very sparse or even absent in TEN.
• Eosinophils are not seen as a rule
18.
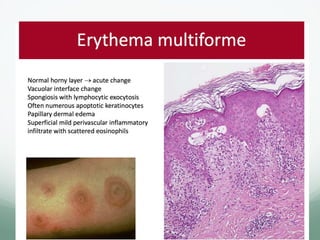
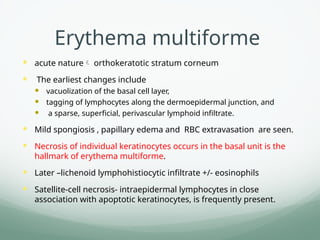
Erythema multiforme
acutenature orthokeratotic stratum corneum
The earliest changes include
vacuolization of the basal cell layer,
tagging of lymphocytes along the dermoepidermal junction, and
a sparse, superficial, perivascular lymphoid infiltrate.
Mild spongiosis , papillary edema and RBC extravasation are seen.
Necrosis of individual keratinocytes occurs in the basal unit is the
hallmark of erythema multiforme.
Later –lichenoid lymphohistiocytic infiltrate +/- eosinophils
Satellite-cell necrosis- intraepidermal lymphocytes in close
association with apoptotic keratinocytes, is frequently present.
19.
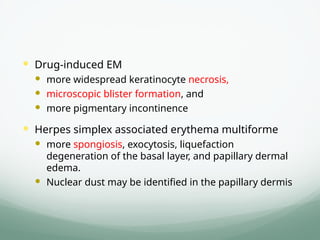
Drug-induced EM
more widespread keratinocyte necrosis,
microscopic blister formation, and
more pigmentary incontinence
Herpes simplex associated erythema multiforme
more spongiosis, exocytosis, liquefaction
degeneration of the basal layer, and papillary dermal
edema.
Nuclear dust may be identified in the papillary dermis
20.
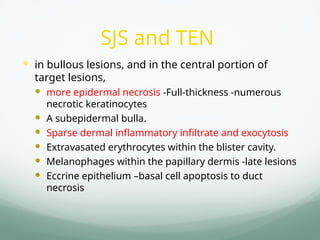
SJS and TEN
in bullous lesions, and in the central portion of
target lesions,
more epidermal necrosis -Full-thickness -numerous
necrotic keratinocytes
A subepidermal bulla.
Sparse dermal inflammatory infiltrate and exocytosis
Extravasated erythrocytes within the blister cavity.
Melanophages within the papillary dermis -late lesions
Eccrine epithelium –basal cell apoptosis to duct
necrosis
21.
Fixed drug eruption.There is obscuration of the dermoepidermal junction with a mixed
inflammatory cell infiltrate composed of lymphocytes
numerous eosinophils and neutrophils (A and B).
Necrotic keratinocytes can be identified throughout all levels of the epidermis (A)and
may tend toward confluence.
A mixed perivascular infiltrate can be present in the deep dermis (C).
22.
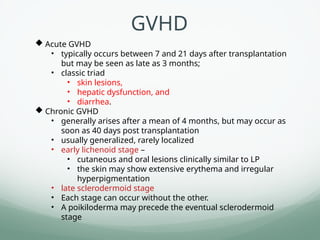
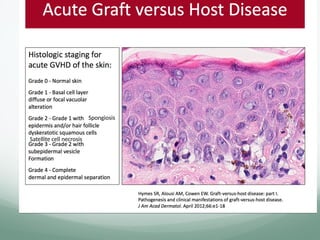
Acute GVHD
•typically occurs between 7 and 21 days after transplantation
but may be seen as late as 3 months;
• classic triad
• skin lesions,
• hepatic dysfunction, and
• diarrhea.
Chronic GVHD
• generally arises after a mean of 4 months, but may occur as
soon as 40 days post transplantation
• usually generalized, rarely localized
• early lichenoid stage –
• cutaneous and oral lesions clinically similar to LP
• the skin may show extensive erythema and irregular
hyperpigmentation
• late sclerodermoid stage
• Each stage can occur without the other.
• A poikiloderma may precede the eventual sclerodermoid
stage
GVHD
23.
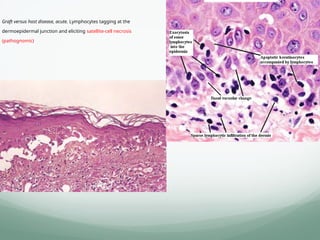
Graft versus hostdisease, acute. Lymphocytes tagging at the
dermoepidermal junction and eliciting satellite-cell necrosis
(pathognomic)
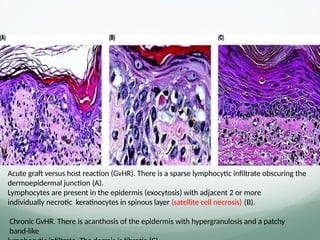
Acute graft versushost reaction (GvHR). There is a sparse lymphocytic infiltrate obscuring the
dermoepidermal junction (A).
Lymphocytes are present in the epidermis (exocytosis) with adjacent 2 or more
individually necrotic keratinocytes in spinous layer (satellite cell necrosis) (B).
Chronic GvHR. There is acanthosis of the epidermis with hypergranulosis and a patchy
band-like
26.
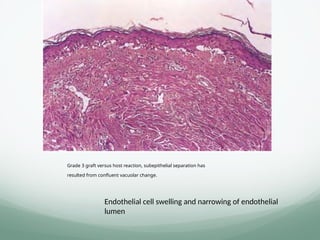
Grade 3 graftversus host reaction, subepithelial separation has
resulted from confluent vacuolar change.
Endothelial cell swelling and narrowing of endothelial
lumen
27.
b) Premature terminaldifferentiation
• Refers to an early development of a thick granular layer and compact
stratum corneum
• A/w dense lichenoid infiltrates of lymphocytes.
• LP is prototype
• Mixed infiltrates:
• Lichenoid drug reaction(eosinophils)
• Keratosis lichenoides chronica (plasma cells)
• Few lymphocytes:
• Dermatomyositis
• Lichenoid GVHD
Dense lymphocytic infiltrates:
• LP
• Lichenoid keratosis
• Lichenoid drug reaction especially
• Photolichenoid
• Acute GVHD
• DLE
• Lichen striatus
28.
c) Irregular epidermalhyperplasia
• variant of permature terminal differentiation
• Show marked irregular epidermal hyperplasia
• Seen in
• Hypertrophic LP
• Verrucous DLE
• Some long- standing lichenoid drug eruptions
29.
d) Interface dermatitiswith psoriasiform
hyperplasia
• Show interface changes as a secondary pathological feature
• Not classified as primary interface dermatitis.
• Lymphocytes and siderophages:
o Lichenoid variant of pigmented purpuric dermatoses
• Eosinophils predominant:
o Urticarial pemphigoid
o Some drug eruptions
• Lymphocytes mostly:
o Mycosis fungoides
o Lichen striatus (True interface dermatitis )
o Fully developed lesions of Pityriasis lichenoides (True interface dermatitis )
o Lichen sclerosus
o Center of porokeratosis
• Plasma cells:
o Secondary syphilis
o Early acrodermatitis chronica atrophicans
30.
e) Interface dermatitiswith epidermal
atrophy
• Represents late atrophic phase of several dermatoses
• Plasma cells:
o Late stage of acrodermatitis chronica atrophicans.
• Band of melanophages:
o Regressing malignant melanoma
o Late pigmented patches of FDE.
• Lymphocytic infiltrate:
o Atrophic LP
o Long-standing lesions of LE, dermatomyositis
o Poikiloderma
o Lichen sclerosus et atrophicus
o Center of old lesions of porokeratosis
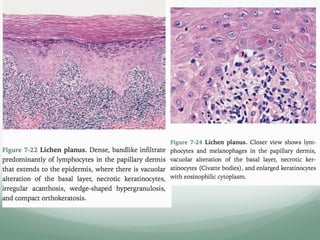
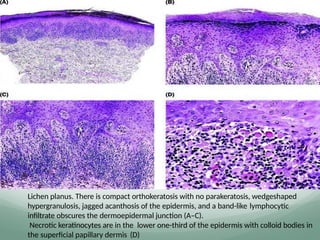
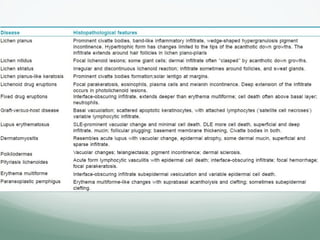
Lichen planus. Thereis compact orthokeratosis with no parakeratosis, wedgeshaped
hypergranulosis, jagged acanthosis of the epidermis, and a band-like lymphocytic
infiltrate obscures the dermoepidermal junction (A–C).
Necrotic keratinocytes are in the lower one-third of the epidermis with colloid bodies in
the superficial papillary dermis (D)
36.
Max Joseph Space/
CaspiniJoseph space
artifactual separation between the
epidermis and the lichenoid infiltrate in
dermis
Lichen planus. Closer view shows
lymphocytes and melanophages in
the papillary dermis, vacuolar
alteration of the basal layer,
necrotic keratinocytes (Civatte
bodies), and enlarged
keratinocytes with eosinophilic
cytoplasm
37.
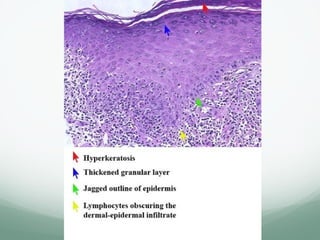
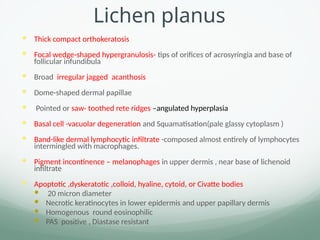
Lichen planus
Thickcompact orthokeratosis
Focal wedge-shaped hypergranulosis- tips of orifices of acrosyringia and base of
follicular infundibula
Broad irregular jagged acanthosis
Dome-shaped dermal papillae
Pointed or saw- toothed rete ridges –angulated hyperplasia
Basal cell -vacuolar degeneration and Squamatisation(pale glassy cytoplasm )
Band-like dermal lymphocytic infiltrate -composed almost entirely of lymphocytes
intermingled with macrophages.
Pigment incontinence – melanophages in upper dermis , near base of lichenoid
infiltrate
Apoptotic ,dyskeratotic ,colloid, hyaline, cytoid, or Civatte bodies
20 micron diameter
Necrotic keratinocytes in lower epidermis and upper papillary dermis
Homogenous round eosinophilic
PAS positive , Diastase resistant
38.
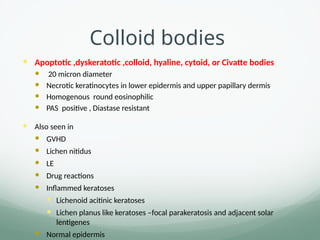
Colloid bodies
Apoptotic,dyskeratotic ,colloid, hyaline, cytoid, or Civatte bodies
20 micron diameter
Necrotic keratinocytes in lower epidermis and upper papillary dermis
Homogenous round eosinophilic
PAS positive , Diastase resistant
Also seen in
GVHD
Lichen nitidus
LE
Drug reactions
Inflammed keratoses
Lichenoid acitinic keratoses
Lichen planus like keratoses –focal parakeratosis and adjacent solar
lentigenes
Normal epidermis
39.
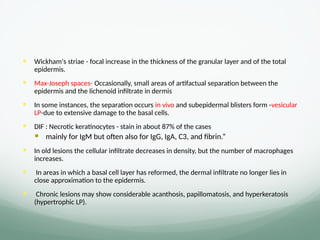
Wickham's striae- focal increase in the thickness of the granular layer and of the total
epidermis.
Max-Joseph spaces- Occasionally, small areas of artifactual separation between the
epidermis and the lichenoid infiltrate in dermis
In some instances, the separation occurs in vivo and subepidermal blisters form -vesicular
LP-due to extensive damage to the basal cells.
DIF : Necrotic keratinocytes - stain in about 87% of the cases
mainly for IgM but often also for IgG, IgA, C3, and fibrin.”
In old lesions the cellular infiltrate decreases in density, but the number of macrophages
increases.
In areas in which a basal cell layer has reformed, the dermal infiltrate no longer lies in
close approximation to the epidermis.
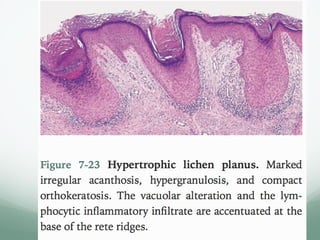
Chronic lesions may show considerable acanthosis, papillomatosis, and hyperkeratosis
(hypertrophic LP).
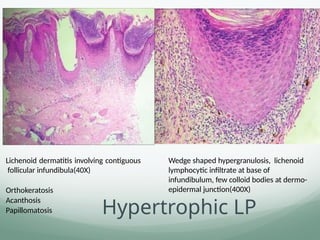
Lichenoid dermatitis involvingcontiguous
follicular infundibula(40X)
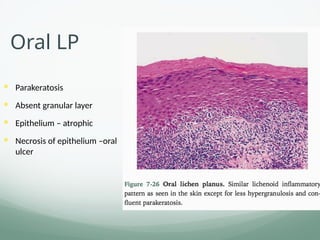
Orthokeratosis
Acanthosis
Papillomatosis
Wedge shaped hypergranulosis, lichenoid
lymphocytic infiltrate at base of
infundibulum, few colloid bodies at dermo-
epidermal junction(400X)
Hypertrophic LP
43.
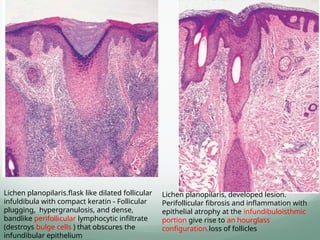
Lichen planopilaris.flask likedilated follicular
infuldibula with compact keratin - Follicular
plugging, hypergranulosis, and dense,
bandlike perifollicular lymphocytic infiltrate
(destroys bulge cells ) that obscures the
infundibular epithelium
Lichen planopilaris, developed lesion.
Perifollicular fibrosis and inflammation with
epithelial atrophy at the infundibuloisthmic
portion give rise to an hourglass
configuration.loss of follicles
44.
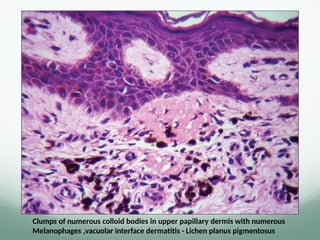
Clumps of numerouscolloid bodies in upper papillary dermis with numerous
Melanophages ,vacuolar interface dermatitis - Lichen planus pigmentosus
45.
DD for LP
Lichenoid drug eruptions
Lichenoid GVHD -Langehans cells decreased , cytotoxic T infiltate in epidermis
Early - perivascular sparse infiltrate
Late –dermal sclerosis
Lichenoid LE
Lichen planus like keratoses -“Focal parakeratosis and adjacent solar lentigines ”
Early SCC in situ – dysplastic keratinocytes
46.
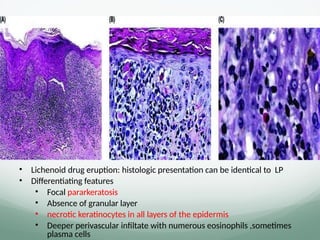
• Lichenoid drugeruption: histologic presentation can be identical to LP
• Differentiating features
• Focal pararkeratosis
• Absence of granular layer
• necrotic keratinocytes in all layers of the epidermis
• Deeper perivascular infiltate with numerous eosinophils ,sometimes
plasma cells
47.
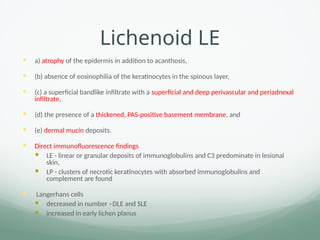
Lichenoid LE
a)atrophy of the epidermis in addition to acanthosis,
(b) absence of eosinophilia of the keratinocytes in the spinous layer,
(c) a superficial bandlike infiltrate with a superficial and deep perivascular and periadnexal
infiltrate,
(d) the presence of a thickened, PAS-positive basement membrane, and
(e) dermal mucin deposits.
Direct immunofluorescence findings
LE - linear or granular deposits of immunoglobulins and C3 predominate in lesional
skin,
LP - clusters of necrotic keratinocytes with absorbed immunoglobulins and
complement are found
Langerhans cells
decreased in number –DLE and SLE
increased in early lichen planus
48.
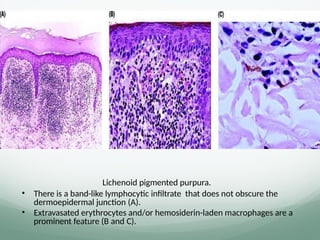
Lichenoid pigmented purpura.
•There is a band-like lymphocytic infiltrate that does not obscure the
dermoepidermal junction (A).
• Extravasated erythrocytes and/or hemosiderin-laden macrophages are a
prominent feature (B and C).
49.
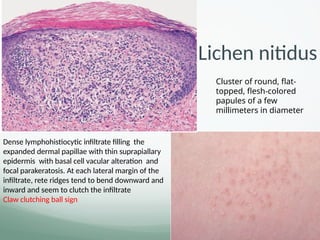
Dense lymphohistiocytic infiltratefilling the
expanded dermal papillae with thin suprapiallary
epidermis with basal cell vacular alteration and
focal parakeratosis. At each lateral margin of the
infiltrate, rete ridges tend to bend downward and
inward and seem to clutch the infiltrate
Claw clutching ball sign
Cluster of round, flat-
topped, flesh-colored
papules of a few
millimeters in diameter
.
Lichen nitidus
51.
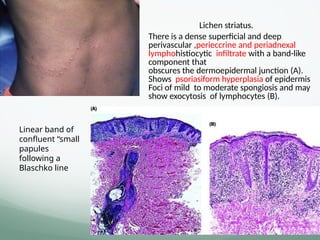
Lichen striatus.
• Thereis a dense superficial and deep
perivascular ,perieccrine and periadnexal
lymphohistiocytic infiltrate with a band-like
component that
obscures the dermoepidermal junction (A).
Shows psoriasiform hyperplasia of epidermis
Foci of mild to moderate spongiosis and may
show exocytosis of lymphocytes (B).
Linear band of
confluent “small
papules
following a
Blaschko line
52.
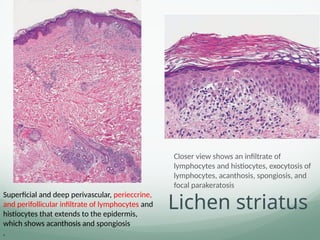
Lichen striatus
Closer viewshows an infiltrate of
lymphocytes and histiocytes, exocytosis of
lymphocytes, acanthosis, spongiosis, and
focal parakeratosis
Superficial and deep perivascular, perieccrine,
and perifollicular infiltrate of lymphocytes and
histiocytes that extends to the epidermis,
which shows acanthosis and spongiosis
.
53.
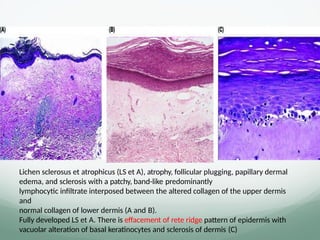
Lichen sclerosus etatrophicus (LS et A), atrophy, follicular plugging, papillary dermal
edema, and sclerosis with a patchy, band-like predominantly
lymphocytic infiltrate interposed between the altered collagen of the upper dermis
and
normal collagen of lower dermis (A and B).
Fully developed LS et A. There is effacement of rete ridge pattern of epidermis with
vacuolar alteration of basal keratinocytes and sclerosis of dermis (C)
56.
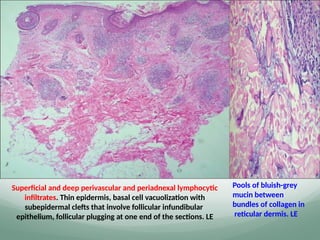
Superficial and deepperivascular and periadnexal lymphocytic
infiltrates. Thin epidermis, basal cell vacuolization with
subepidermal clefts that involve follicular infundibular
epithelium, follicular plugging at one end of the sections. LE
Pools of bluish-grey
mucin between
bundles of collagen in
reticular dermis. LE
57.
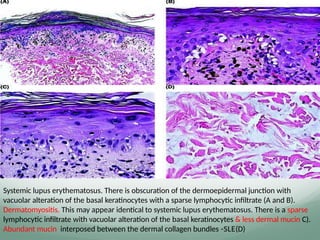
Systemic lupus erythematosus.There is obscuration of the dermoepidermal junction with
vacuolar alteration of the basal keratinocytes with a sparse lymphocytic infiltrate (A and B).
Dermatomyositis. This may appear identical to systemic lupus erythematosus. There is a sparse
lymphocytic infiltrate with vacuolar alteration of the basal keratinocytes & less dermal mucin C).
Abundant mucin interposed between the dermal collagen bundles -SLE(D)
58.
Discoid lupus erythematosus.There is a superficial and deep perivascular and periadnexal
lymphocytic infiltrate with vacuolar alteration of the basal keratinocytes (A and B).
A dense lymphocytic infiltrate surrounds the follicular adnexae with obscuration of the
epithelial-stromal junction(C). Note the marked thickening of the basement membrane (D)
59.
Tumid LE –D/DDifferentiating features
1.Lymphocytic
lymphoma
• atypical lymphocytes
• interstitial distribution (“Indian filing”), and
• Do not surround pilosebaceous units
2.Lymphocytoma cutis • Heavier infiltrate
• Interstitial component,
• Do not surround pilosebaceous units
• Often contains an admixture of larger, paler lymphocytes
arranged in lymphoid follicles, mimicking germinal center
formation
3.plaque type of
polymorphous light
eruption
• prominent band of papillary dermal edema.
• The infiltrate is more intense in the superficial dermis than in
deep dermis and is occasionally admixed with neutrophils.
• No folliculocentric arrangement and
• No stromal mucin deposition
4.Jessner lymphocytic
infiltration of the skin
• plasma cells and mucin are absent.
• presence of increased numbers of B lymphocytes in the infiltrate
5.Lues
6.Lyme’s disease
IHC , silver stain
No mucin deposition
60.
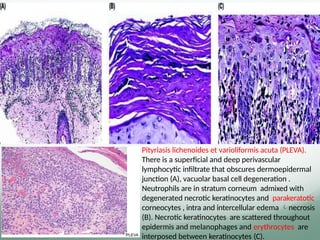
Pityriasis lichenoides etvarioliformis acuta (PLEVA).
There is a superficial and deep perivascular
lymphocytic infiltrate that obscures dermoepidermal
junction (A), vacuolar basal cell degeneration .
Neutrophils are in stratum corneum admixed with
degenerated necrotic keratinocytes and parakeratotic
corneocytes , intra and intercellular edema necrosis
(B). Necrotic keratinocytes are scattered throughout
epidermis and melanophages and erythrocytes are
interposed between keratinocytes (C).
61.
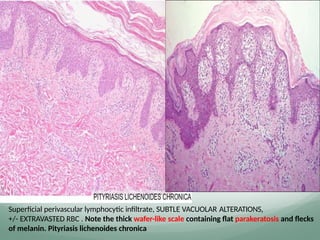
Superficial perivascular lymphocyticinfiltrate, SUBTLE VACUOLAR ALTERATIONS,
+/- EXTRAVASTED RBC . Note the thick wafer-like scale containing flat parakeratosis and flecks
of melanin. Pityriasis lichenoides chronica
62.
D/D for PLEVAand PLC
Pityriasis rosea
Vesicular insect bites
Numerous eosinophils in a vertically oriented dermal infiltrate are more
commonly seen in insect bites
Subacute eczematous dermatitis
PLEVA vs PR, subacute eczema
The presence of a deeper inflammatory infiltrate,
extensive epidermal necrosis, and
the absence of intraepidermal spongiotic microvesicles
Guttate psoriasis
Lymphomatoid papulosis
#39 A few eosinophils and/or plasma cells may be seen in close approximation to the epidermis, but these are rare except in some examples of hypertrophic LP.






















![Linear_Lesions_In_Dermatology [1].pptxhhh](https://cdn.slidesharecdn.com/ss_thumbnails/linearlesionsindermatology1-251122025615-0177ddce-thumbnail.jpg?width=640&height=640&fit=bounds)






























