Downloaded 352 times
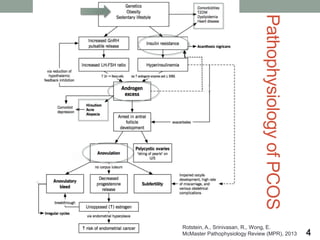
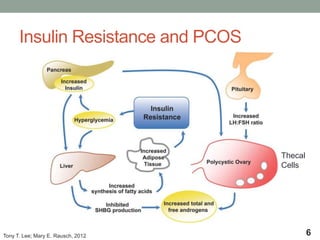
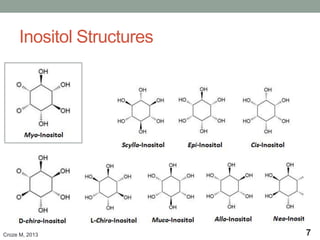

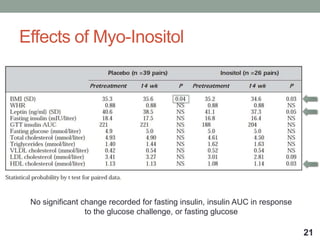
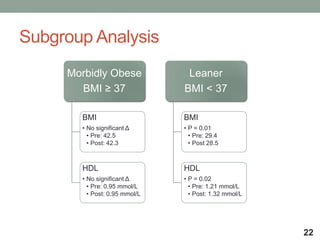
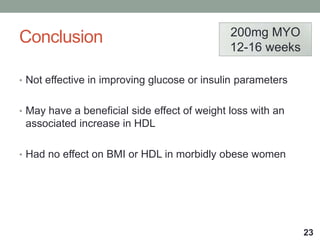
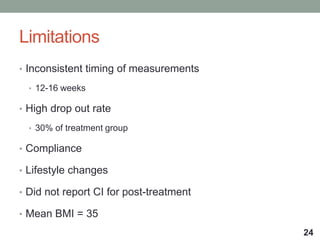
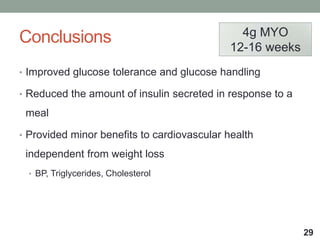
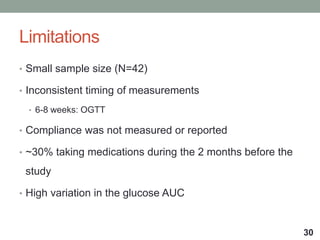
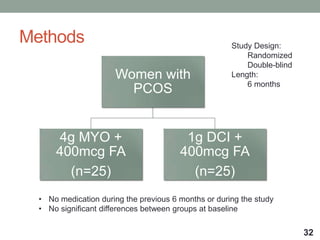
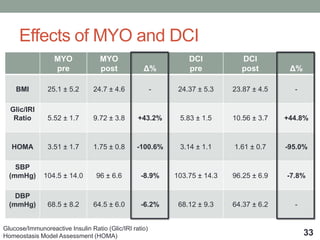
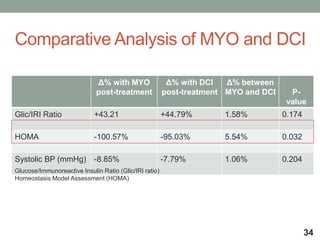
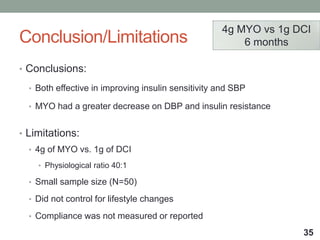
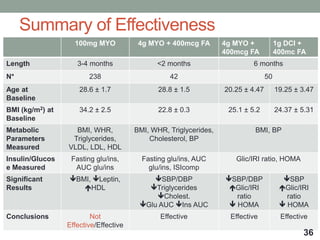

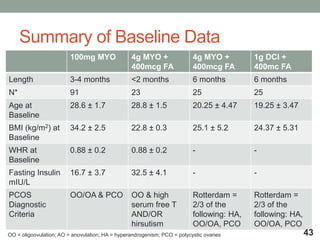
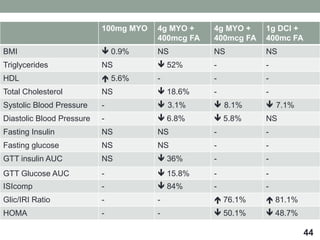
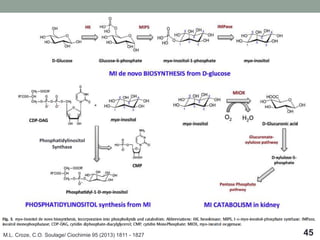

The document evaluates the effectiveness of inositol supplementation in improving insulin sensitivity and metabolic parameters in women with polycystic ovary syndrome (PCOS). Studies indicate that while some formulations of myo-inositol show potential benefits, such as improved glucose tolerance and possible weight loss, overall effectiveness varies, and limitations include small sample sizes and inconsistent results. Further research is necessary to clarify the impact of inositol on PCOS and consider lifestyle interventions as a primary treatment option.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










