• Immunity -is the state of being resistant to
injury particularly by poisons, foreign bodies
and invading organisms due to the presence of
antibodies
• Antigen – is a substance that when introduced
into the body induces the formation of
antibodies or reacts with them
• Antibody – is a substance produced by certain
cells in the presence of a specific antigen. The
antibody combines with the antigen to
neutralise or inhibit or destroy it.
3.
Types of Immunity
i.Natural Immunity
• This can be passive or active
a. Active Natural Immunity
• A person suffers from a specific disease
develops antibodies against that specific
disease eg a person who suffers from
smallpox and recovers from it develops
antibodies against smallpox.
4.
b. Passive NaturalImmunity
• This refers to the transplacental passage
of antibodies from the mother to her
unborn child during the latter part of
pregnancy
• The baby’s body does not develop any
antibodies eg mother immunized against
tetanus will pass her antibodies to the
unborn baby
5.
ii. Acquired orArtificial Immunity
• Is an artificially induced immunity (man-
made procedure)
• Can be either Active or Passive
a. Active Artificial Immunity
• Is the immunity resulting from the
injection of antigens (vaccines) of a
specific disease
• These antigens act as stimulus which
initiates antibody production against that
specific antigen
6.
• On subsequentvisitation by this same
antigen, these antibodies produced will
assist in the body’s defence
• Killed and attenuated (weakened) strains
of bacteria and viruses are used for
immunisations against many diseases eg
TB, Measles etc
7.
Advantages of ActiveImmunity
• The antibodies are the person’s own and
the body then remembers how each
particular antibody was made.
• If a person is again exposed to an
infection he/she has already being
vaccinated against, the body will very
quickly make more antibodies to fight off
the microorganisms, usually before they
even start growing in the body
8.
Disadvantage
• It doesnot give the immediate protection as it
takes some days for the body to develop
antibodies
b. Passive Artificial Immunity
• It refers to the original production of antibodies
in some other individuals either human or
mammals
• The person is injected already made antibodies
• It is passive because the body does not develop
antibodies
9.
Advantages
• The personreceiving the antibodies does
not have to wait for his own body to
produce them
• The person has immediate assistance in
fighting against the infection
10.
Disadvantages
• Immunity isshort lasting as the body
cannot remember to produce antibodies
when re-infection occurs
• The body may react to these injected
antibodies by producing other antibodies.
Eg a person with open wounds from
accident is given anti-tetanus serum
11.
IMMUNISATION
• Is aprocedure whereby a vaccine is
administered to an individual in order to
stimulate his body to produce its own antibodies
against a specific disease.
• A Vaccine is a suspension of attenuated or
dead organisms used as antigens
• These antigens are too weak to cause the
disease
• These antigens nevertheless stimulate an
immune response by developing antibodies
against a specific antigen
12.
Types of Vaccine
a.Active Vaccine
• This stimulates the body to produce its
own antibodies
• Immunity is slow to develop but is long-
lasting eg DPT, OPV, Measles, Mumps,
Pneumococci,Hepatitis B, HIB, Rubella,
Rotavirus
13.
• Is alsogrouped into:
i. Live Attenuated Vaccine
• These can be prepared from harmless, live
microbes
• The weakened organisms will produce a mild
infection of little danger to the host
• Is best for long term protection
• Often fewer doses are required eg BCG,
Measles (1dose), Polio (4 doses are required),
yellow fever
14.
ii. Dead orKilled Vaccine
• Are prepared from dead microbes
• Are however capable of stimulating the
body to produce antibodies against the
specific antigens
• Immunity lasts only for a few years and
needs to be boosted whenever there is a
danger of contracting a disease eg
Pertusis (3doses), Cholera, Hepatitis B,
Plague
15.
iii. Toxoids
• Vaccinesare made from detoxified Toxins
• These inactivated, harmless toxins are
capable of stimulating the body to develop
antibodies against the specific antigen
• The vaccine is called Toxoid
• Also less strong hence needs more doses
eg Tetanus toxoid (5doses), Diphtheria
toxoid
16.
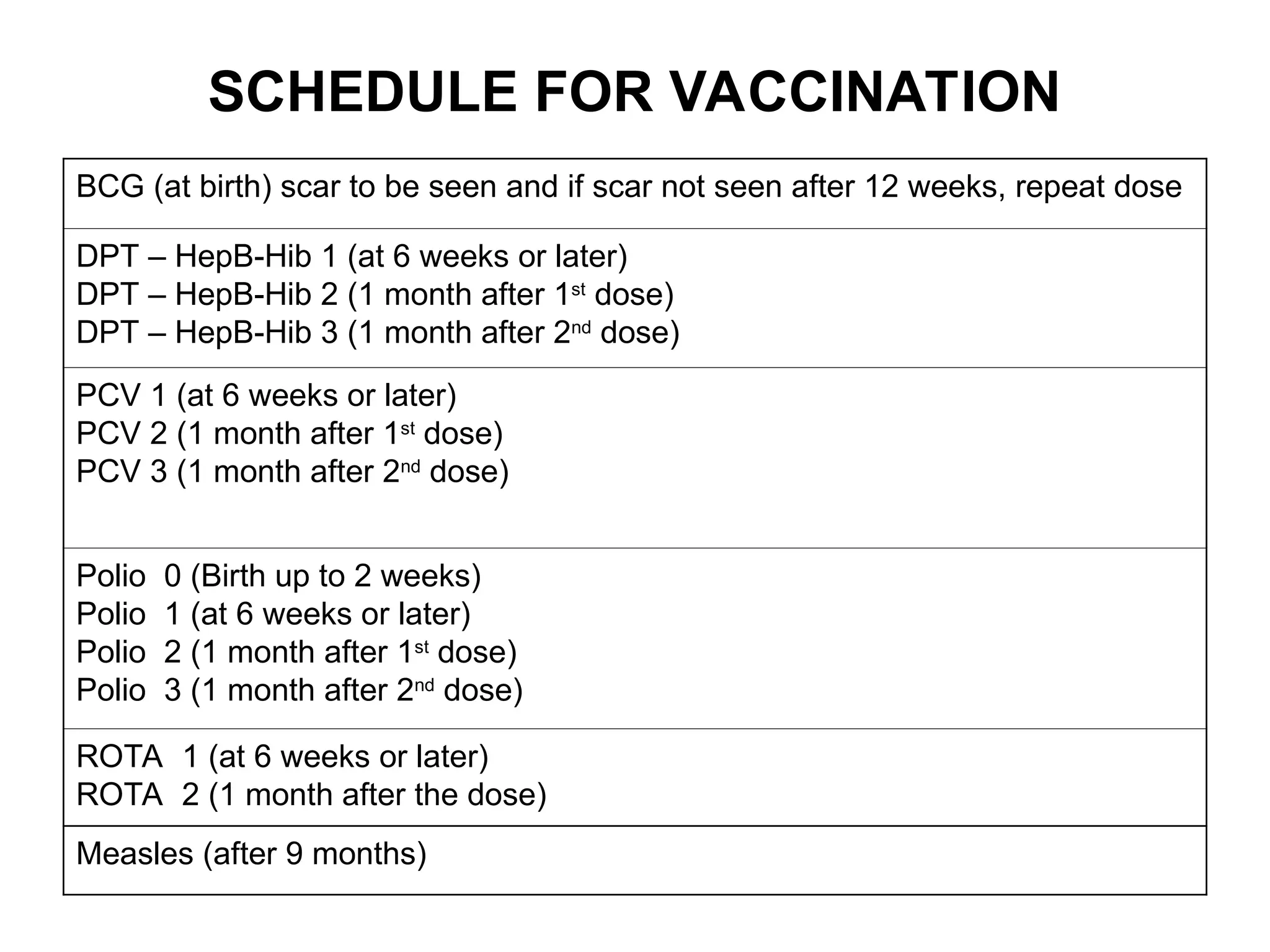
SCHEDULE FOR VACCINATION
BCG(at birth) scar to be seen and if scar not seen after 12 weeks, repeat dose
DPT – HepB-Hib 1 (at 6 weeks or later)
DPT – HepB-Hib 2 (1 month after 1st
dose)
DPT – HepB-Hib 3 (1 month after 2nd
dose)
PCV 1 (at 6 weeks or later)
PCV 2 (1 month after 1st
dose)
PCV 3 (1 month after 2nd
dose)
Polio 0 (Birth up to 2 weeks)
Polio 1 (at 6 weeks or later)
Polio 2 (1 month after 1st
dose)
Polio 3 (1 month after 2nd
dose)
ROTA 1 (at 6 weeks or later)
ROTA 2 (1 month after the dose)
Measles (after 9 months)
17.
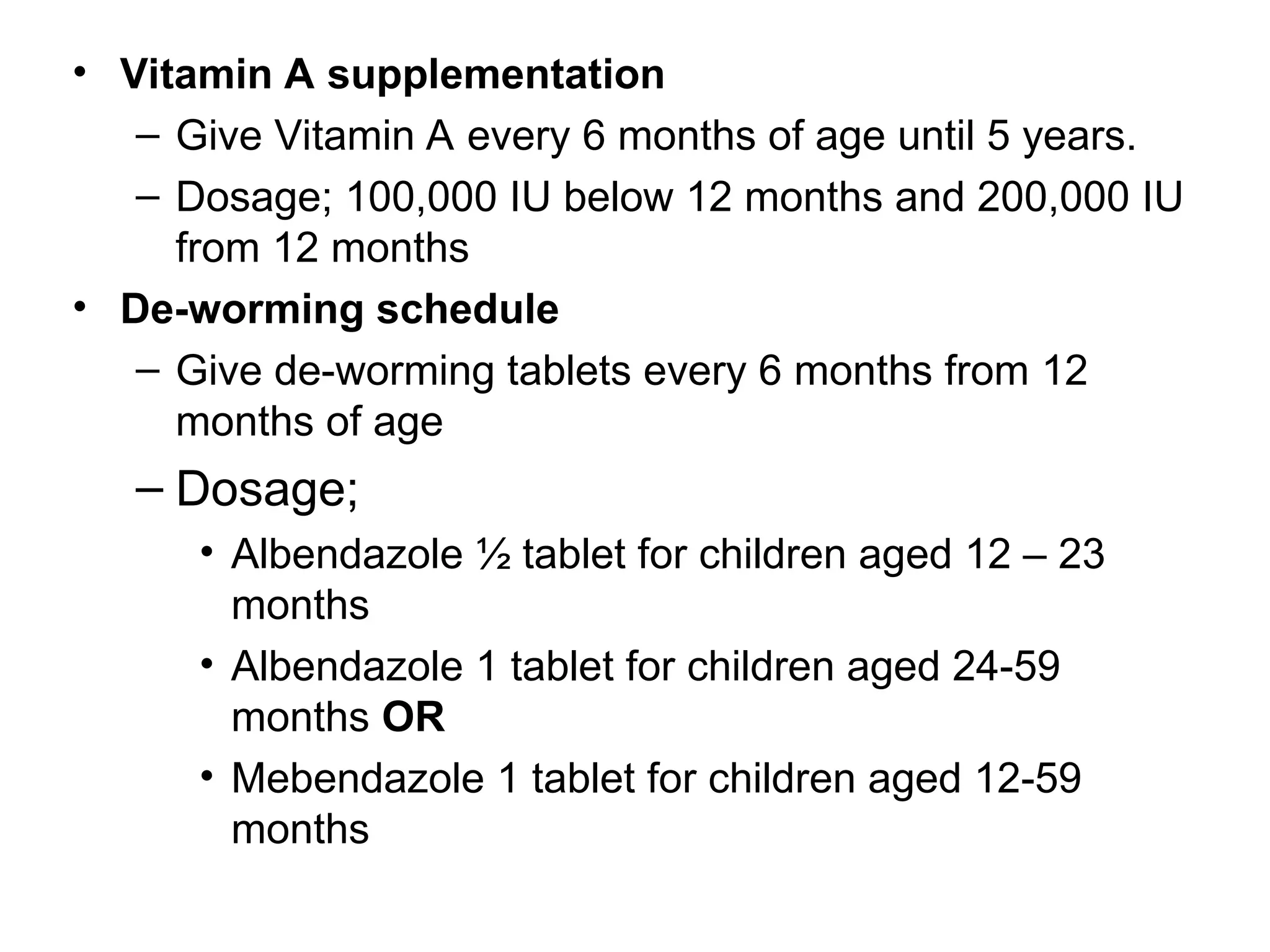
• Vitamin Asupplementation
– Give Vitamin A every 6 months of age until 5 years.
– Dosage; 100,000 IU below 12 months and 200,000 IU
from 12 months
• De-worming schedule
– Give de-worming tablets every 6 months from 12
months of age
– Dosage;
• Albendazole ½ tablet for children aged 12 – 23
months
• Albendazole 1 tablet for children aged 24-59
months OR
• Mebendazole 1 tablet for children aged 12-59
months
18.
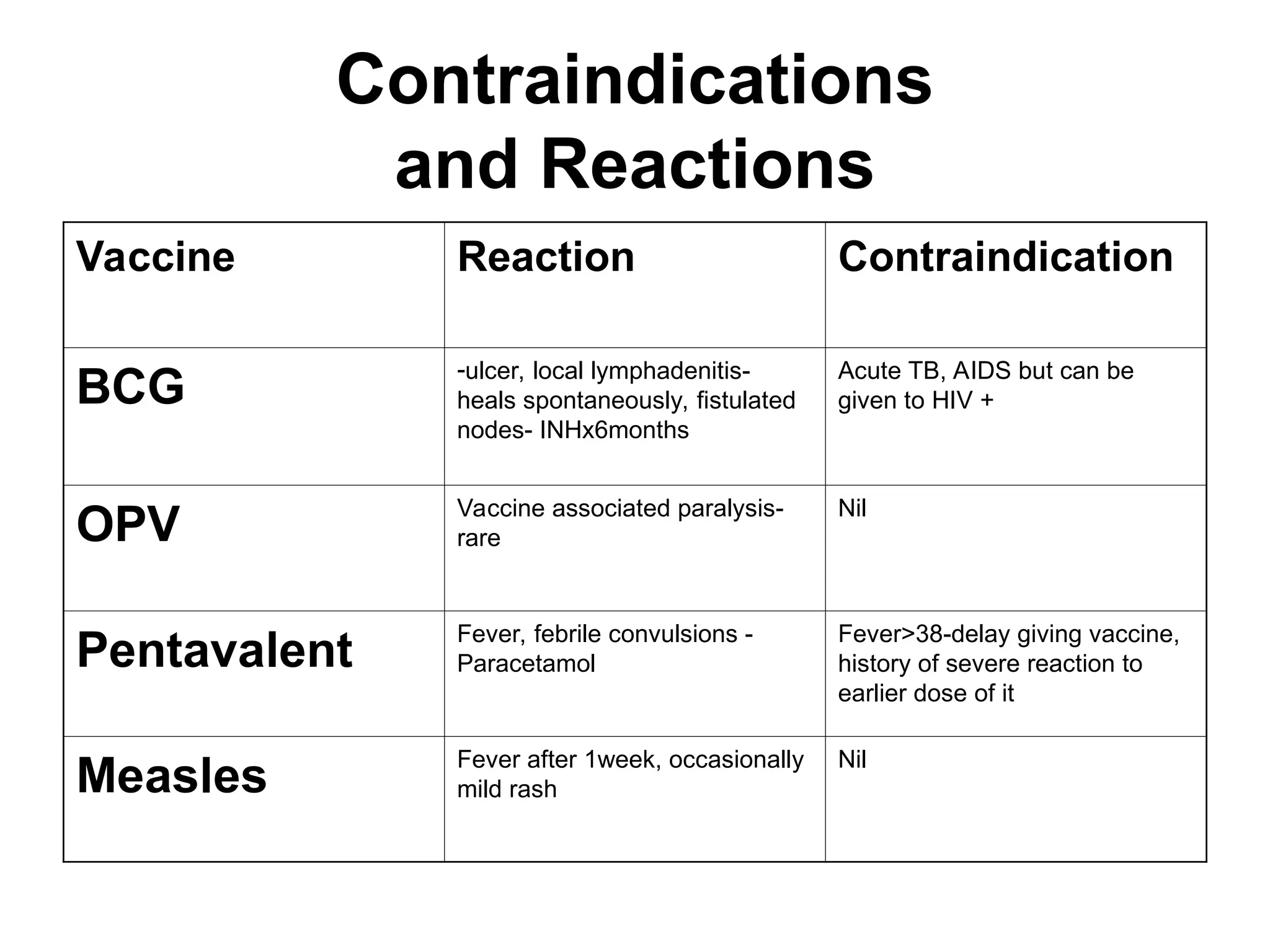
Contraindications
and Reactions
Vaccine ReactionContraindication
BCG
-ulcer, local lymphadenitis-
heals spontaneously, fistulated
nodes- INHx6months
Acute TB, AIDS but can be
given to HIV +
OPV
Vaccine associated paralysis-
rare
Nil
Pentavalent Fever, febrile convulsions -
Paracetamol
Fever>38-delay giving vaccine,
history of severe reaction to
earlier dose of it
Measles Fever after 1week, occasionally
mild rash
Nil
19.
EXPANDED PROGRAM ON
IMMUNISATION(EPI)
Background to EPI
• During the late 70’s and early 80’s, 5
million children in developing countries
died and another 5 million were disabled
annually due to the six childhood vaccine
preventable diseases
• In May 1974, WHO established the EPI
20.
Goal of EPI
•The goal is to reduce morbidity and
mortality rates from vaccine preventable
diseases such as measles, TB,
Poliomyelitis, Diphtheria, Pertusis,
Haemophilus Influenza B and Hepatitis B
virus infections
21.
EPI in Malawi
•The second Malawi National Health Plan
of 1973 to 1988 had the improvement of
existing health services as one of its
priorities
• Prior to 1973, only Smallpox vaccination
was given on a large scale, while BCG
and DPT were provided in a few health
centres
22.
Min-Plan – 1074to 1978
• Within the 15 year National Health Plan
was a 5 year Min plan
• The min-plan was designed to strengthen
maternal and child health (MCH) services
• Its objectives were:
- To improve immunisation coverage
- Provide health and nutrition in children,
pregnant women and nursing mothers
- To promote family life education
23.
• In 1979,Malawi launched the Expanded
Program on Immunisation and has since fully
integrated in the preventive health services
• Immunisation activities are carried along with
other components of the essential health care
package such as
- Growth monitoring
- Family planning
- Nutrition etc
24.
Activities for strengtheningthe
EPI program
• Pre and in-service training of health
personnel
• Consolidating and maintaining cold chain
system to ensure vaccine potency and
improve vaccine distribution system
• Increasing public awareness and
participation about EPI
25.
Organisation of EPIIn Malawi
Central Level
• Is headed by the National Program
Manager who reports to the controller of
preventive health services
• The Manager is assisted by the National
Logistic officer, the National EPI store/cold
chain officer, the National data officer, 2
regional coordinators and 2 cold chain
technicians (north and south)
26.
District Level
• Apublic Health officer and a Community
health Nurse manage EPI services
• Functionally, are called District Maternal
and Child Health/EPI Coordinators and
report to the District Health Officer
• These are assisted by the District cold
chain technicians
27.
Health Centre Level
•May be assigned to any cadre available
there at the centre
Community Level
• The Health Surveillance Assistants live in
the villages amongst the people they treat
28.
• Immunisation servicesare offered at the:
- Static units
- Outreach/mobile clinics
- National immunisation days
29.
Funding
• Funding forthe procurement of cold chain
supplies and vaccines comes from many
external donors and is channelled through
both UNICEF, DFID and WHO etc
30.
Immunisation Policy forMalawi
• Immunise all children less than 12months old
• Immunise pregnant women and all females of 14
to 45 years
• Increase public awareness through health
education and motivation on the need for
immunisation
• Use every contact of a child with the health
delivery system as an opportunity to check the
child’s immunisation status
31.
TEN COMMANDMENTS OF
IMMUNISATION
•Never use expired vaccines
• Immunise at every opportunity, especially
on admission to hospital
• Always ask for the health passport
• Don’t spread HIV-always use sterile needle
and syringe for each injection
• Monitor the cold chain
• Keep all vaccines at the correct
temperature
32.
• Never freezePentavalent/tetanus toxoid
• Never use sterile water for dilution
• It is safe to give all the vaccines at same
time at different body sites
• There are very few contraindications to
vaccination
33.
How to Give
•BCG (0.05ml if <12months, 0.1ml if
>12months) IM in the right upper arm
• Pentavalent 0.5mls IM in lateral thigh
• OPV 2drops on the tongue
• Measles 0.5ml deep subcutaneous on
lateral thigh. Give at 6-9months during
measles outbreak, if admitted to the
hospital or refugees
34.
Storage and Handlingof
Vaccines
• Define cold chain
• Mention factors that can reduce the
potency of vaccines
• List equipment and supplies used in cold
chain
• Describe the steps on how to store
vaccines
35.
• Cold Chainis a means by which vaccines are
continuously maintained at safe temperatures
from time of manufacture until the health worker
uses them
• Includes every stage of transportation and
storage at international, national, regional,
district, health centres down to mobile clinics
• If vaccines are exposed, they will not give
effective protection
• Once potency is lost , cannot be regained
36.
Factors that canreduce the
potency of vaccines
• Heat
• Light
• Freezing
• Vigorous shaking of vaccines
37.
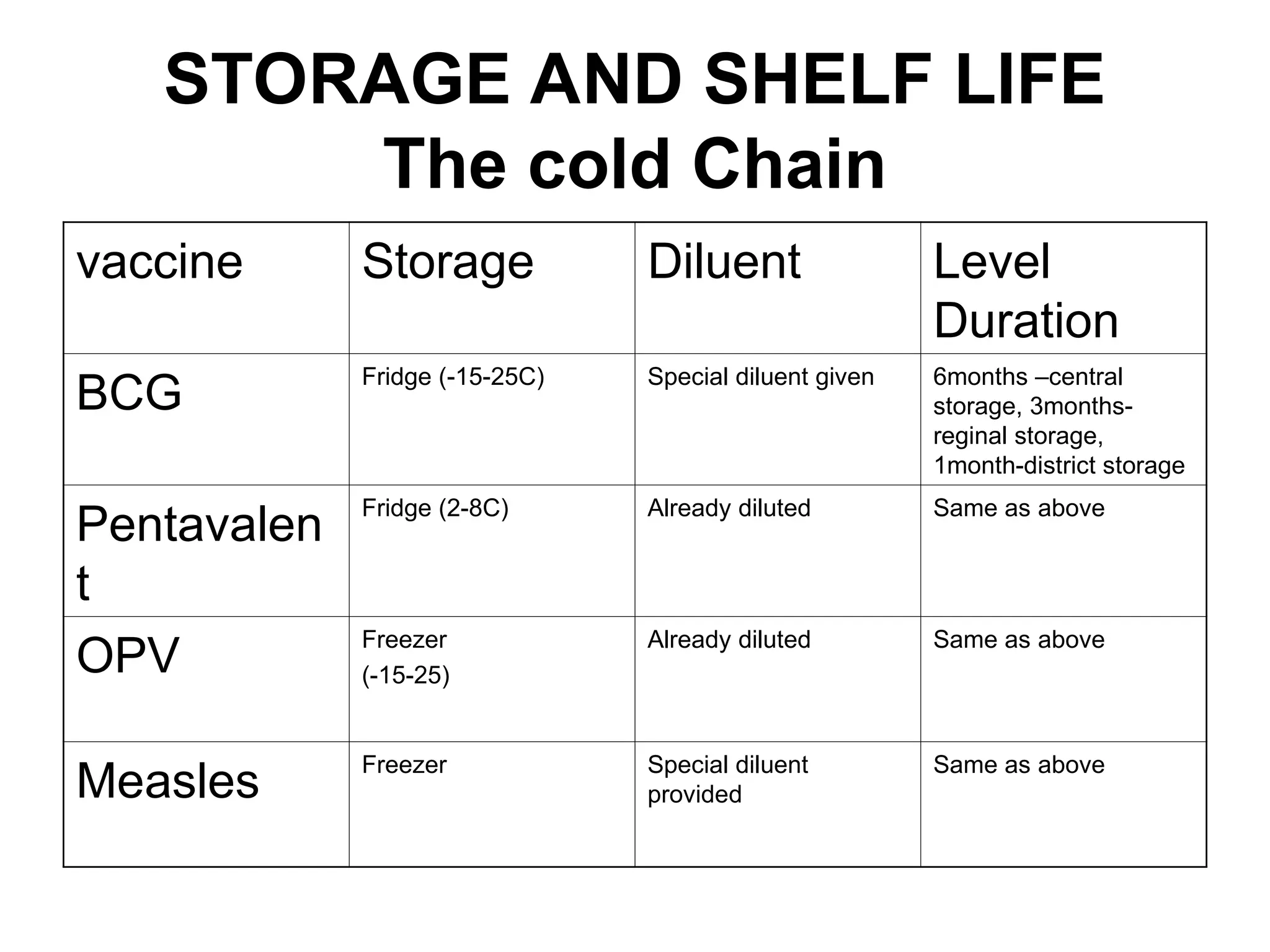
STORAGE AND SHELFLIFE
The cold Chain
vaccine Storage Diluent Level
Duration
BCG
Fridge (-15-25C) Special diluent given 6months –central
storage, 3months-
reginal storage,
1month-district storage
Pentavalen
t
Fridge (2-8C) Already diluted Same as above
OPV
Freezer
(-15-25)
Already diluted Same as above
Measles Freezer Special diluent
provided
Same as above
38.
NB
• All vaccinesare heat sensitive and hence
maintain their cold chain from
manufacturers to use to preserve their
potency
39.
EPI TARGET DISEASES
•These are the EPI target diseases
- TB
- Diphtheria
- Pertusis
- Tetanus
- Polio
- Hepatitis B
- Haemophilus Influenza
- Measles
• Vitamin A deficiency included
40.
VITAMIN A DEFICIENCY
•Vitamin A is a substance that is required
by the human body for the following
functions:
- Strengthening resistance to infection
- Promotes growth
- Protects the cornea
41.
• The bodycannot make Vitamin A, so all of the
Vitamin A we need come from the food we eat
like: Breast milk, liver, eggs, meat, fish, milk
products, yellow and orange fruits, yellow and
orange vegetables, dark green leafy vegetables
etc
• Vitamin A deficiency occurs when the person
does not take enough food containing Vitamin A
or when it is highly demanded by the body in
case of illness, pregnancy, lactation and during
rapid growth























































![Presentation1 CPAP VK [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/presentation1cpapvkautosaved-240916053956-61159a7a-thumbnail.jpg?width=640&height=640&fit=bounds)























