Download to read offline


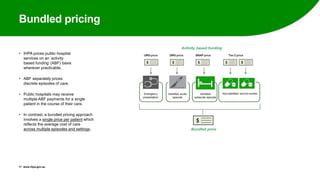
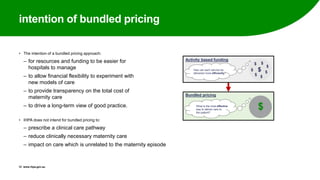
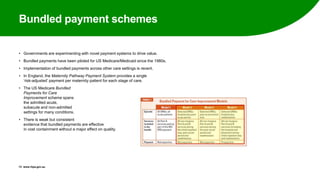
















The Independent Hospital Pricing Authority (IHPA) is committed to transparency and efficiency in hospital pricing, focusing on Activity Based Funding (ABF) and bundled pricing to streamline costs and improve care management. The IHPA consulted stakeholders on implementation for maternity care, proposing that bundled pricing includes all stages and types of maternity services, reflecting average costs across care types while allowing flexibility for hospitals. Key challenges include establishing data consistency for cost comparisons and identifying risk factors that influence service delivery and costs.


































































