A CASE OF
HYPONATREMIA
UNIT3
CHIEF:PROFESSOR:G.SATHISHKUMAR MD
ASSISTANT PROFESSOR:
DR.A.JOSEPH PANNER SELVAM DNB
DR.L.MUTHUMANI DA, MD
1
2.
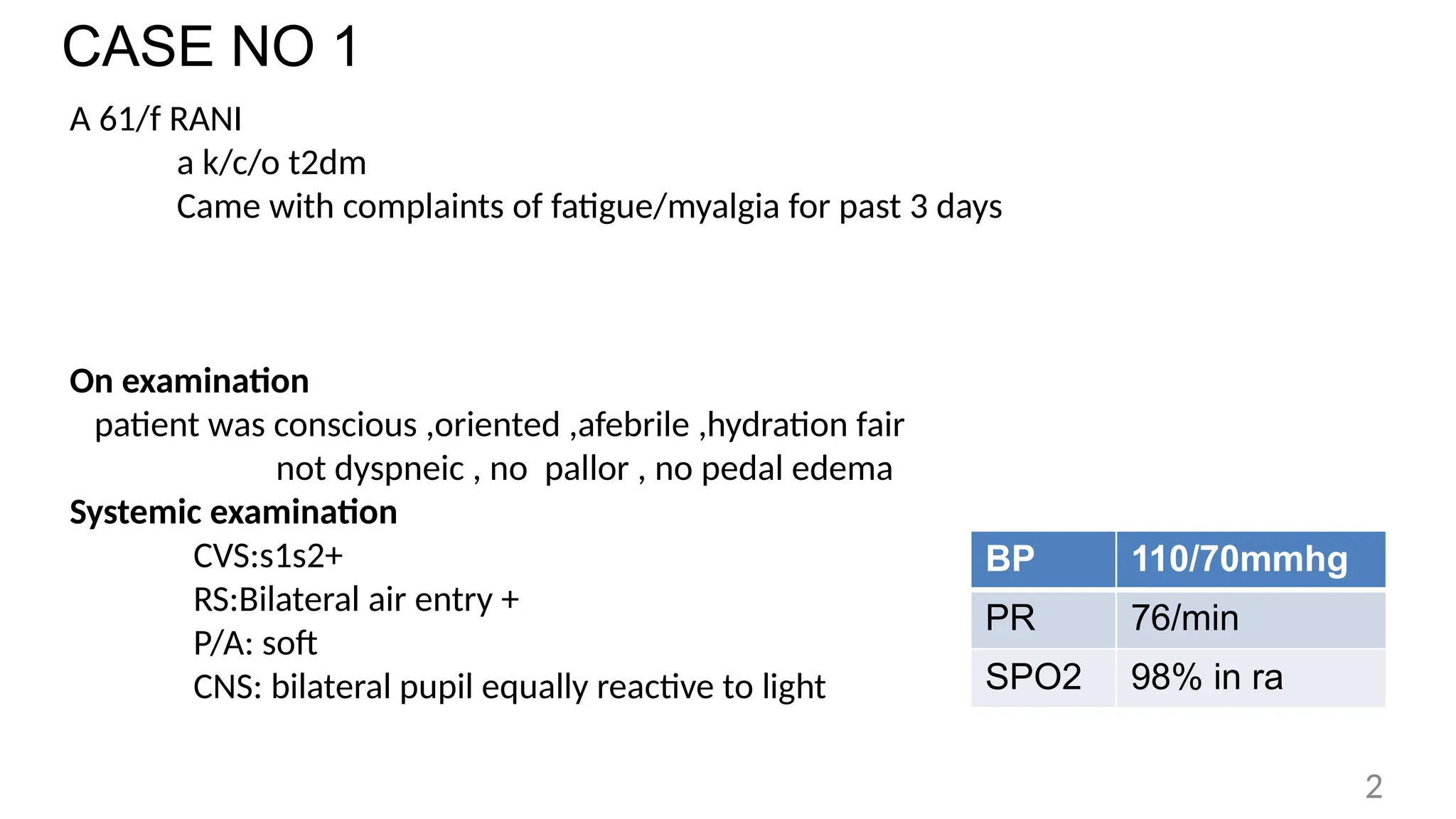
CASE NO 1
A61/f RANI
a k/c/o t2dm
Came with complaints of fatigue/myalgia for past 3 days
On examination
patient was conscious ,oriented ,afebrile ,hydration fair
not dyspneic , no pallor , no pedal edema
Systemic examination
CVS:s1s2+
RS:Bilateral air entry +
P/A: soft
CNS: bilateral pupil equally reactive to light
BP 110/70mmhg
PR 76/min
SPO2 98% in ra
2
HYPEROSMOLAR HYPONATREMIA
• Osmoticallyactive solutes other than sodium accumulates in ECF , drawing water
into ECF and diluting the sodium content.
CAUSES :Hyperglycemia , post transurethral resection of prostate syndrome –
transient hyponatremia – bladder irrigation –glycine, sorbitol, mannitol.
Hyponatremia associated with severe hyperglycemia is not considered
pseudohyponatremia. It is the result of sodium dilution due to water shift from the
intracellular compartment
serum sodium decreases by about 1.6 mEq/l for every 100 mg/dl of glucose
above the normal range which is around 100 mg/dl
Corrected sodium = measured sodium + [1.6 x (measured glucose -100/100)]
5
6.
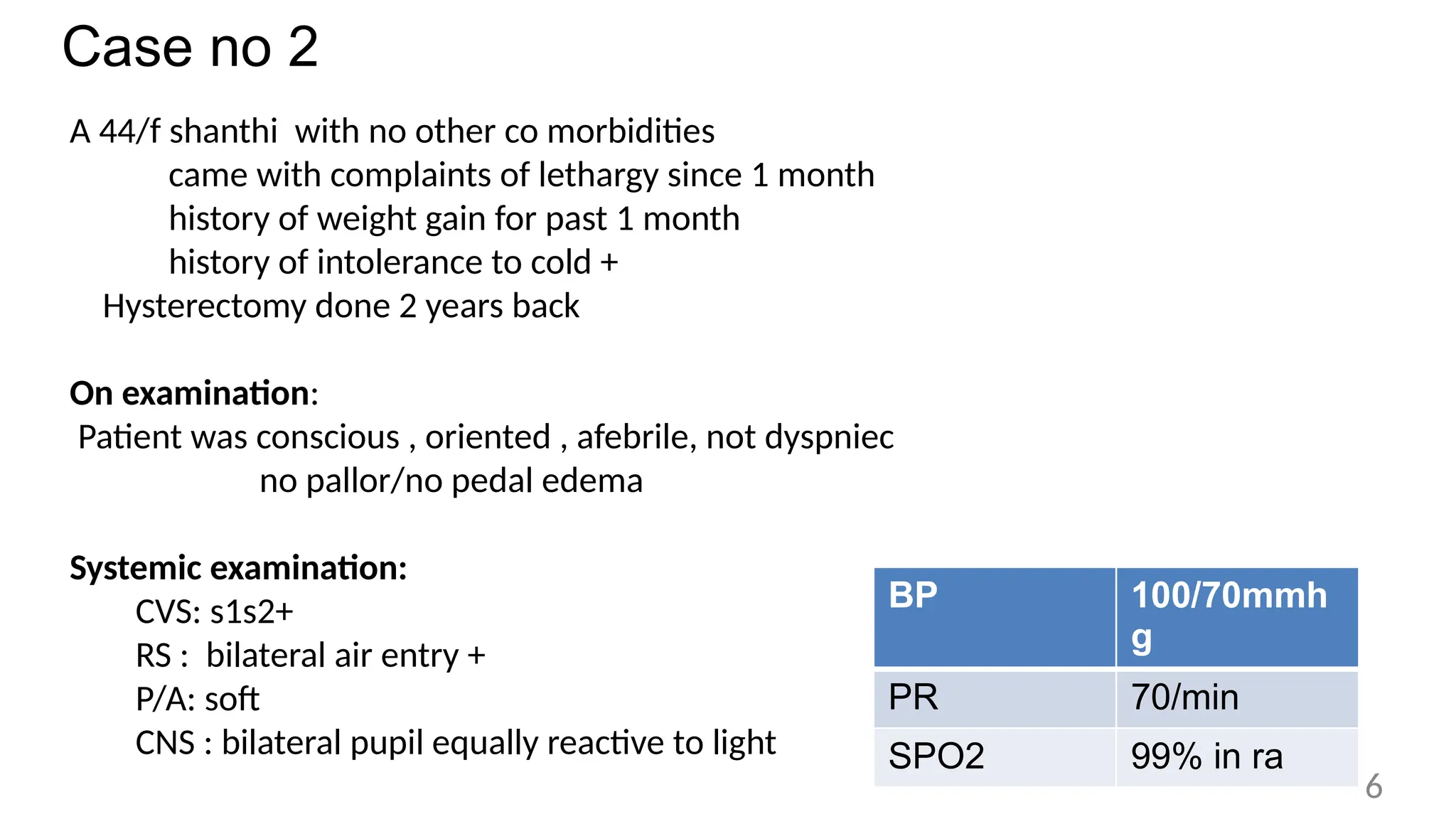
Case no 2
A44/f shanthi with no other co morbidities
came with complaints of lethargy since 1 month
history of weight gain for past 1 month
history of intolerance to cold +
Hysterectomy done 2 years back
On examination:
Patient was conscious , oriented , afebrile, not dyspniec
no pallor/no pedal edema
Systemic examination:
CVS: s1s2+
RS : bilateral air entry +
P/A: soft
CNS : bilateral pupil equally reactive to light
BP 100/70mmh
g
PR 70/min
SPO2 99% in ra
6
7.
TOTAL COUNT 4300
HB9.8 g/dl
PLATELET 234000 lakhs
RBS 186
UREA/
CREATININE
24/ 0.6
T.BIL 0.9
OT/PT 18/ 22
ALP 86
SERUM
PROTEIN/ALBUM
IN
6.1/3.6
SERUM NA/K 124/ 4.1
SERUM
OSM
266 Mosm/l
URINE
OSM
146 mosm/l
URINE NA 28 mEq/l
URINE K 12 mEq/l
TSH 36.4 mIU/ml(0.45 -4.5)
FT4 0.3ng/dl (0.8 – 1.8)
FT3 0.9pg/ml(1.4 -4.4)
7
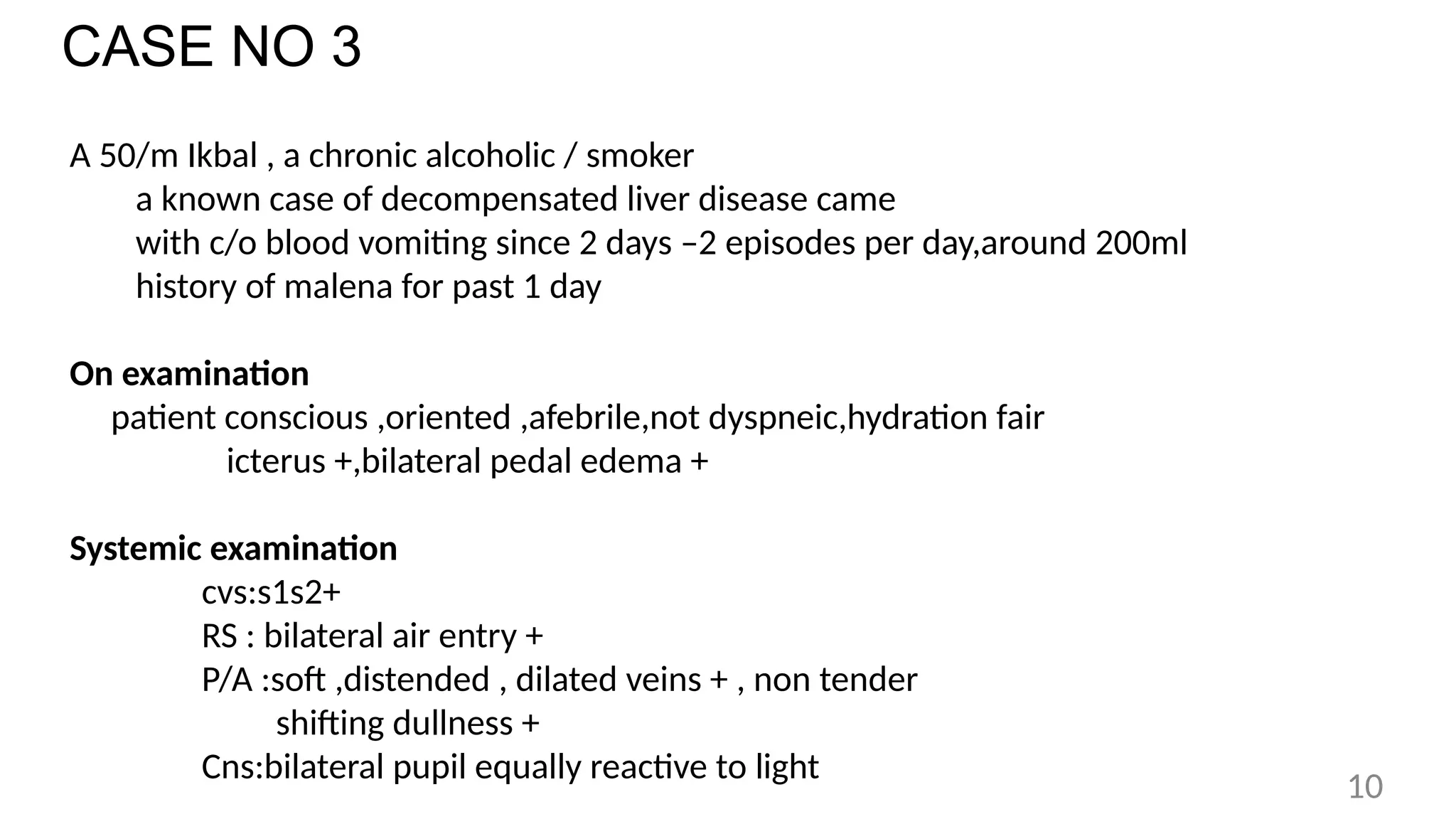
CASE NO 3
A50/m Ikbal , a chronic alcoholic / smoker
a known case of decompensated liver disease came
with c/o blood vomiting since 2 days –2 episodes per day,around 200ml
history of malena for past 1 day
On examination
patient conscious ,oriented ,afebrile,not dyspneic,hydration fair
icterus +,bilateral pedal edema +
Systemic examination
cvs:s1s2+
RS : bilateral air entry +
P/A :soft ,distended , dilated veins + , non tender
shifting dullness +
Cns:bilateral pupil equally reactive to light
10
11.
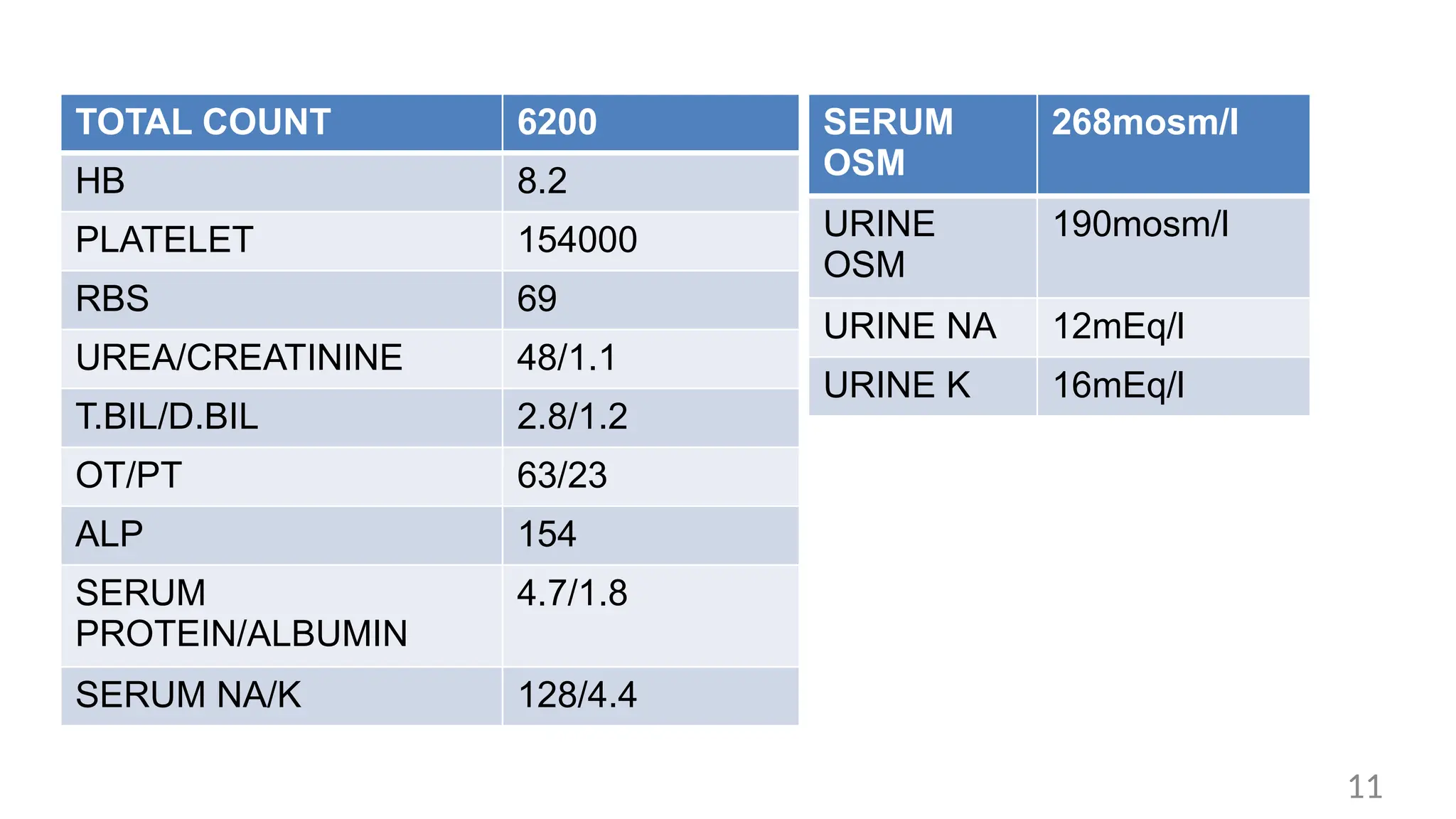
TOTAL COUNT 6200
HB8.2
PLATELET 154000
RBS 69
UREA/CREATININE 48/1.1
T.BIL/D.BIL 2.8/1.2
OT/PT 63/23
ALP 154
SERUM
PROTEIN/ALBUMIN
4.7/1.8
SERUM NA/K 128/4.4
SERUM
OSM
268mosm/l
URINE
OSM
190mosm/l
URINE NA 12mEq/l
URINE K 16mEq/l
11
HYPERVOLEMIC HYPONATREMIA
Patients havesigns of hypervolemia – peripheral edema and ascites
Causes – Heart failure , liver cirrhosis , renal diseases
Mechanism – due to decrease in effective circulating volume the kidney
receives a lesser amount of cardiac output which increase in ADH secretion
and water retention
Hyponatremia may be dilutional ,urine sodium is low unless patient is on
diuretics
Hyponatremia in primary polydipsia , beer protomania is due to excess intake
of water.
Treatment – loop diuretics, salt and fluid restrictions
13
14.
Case no.4
A 20yr/femalesangeetha Came with
Complaints of fever for past 2days -high grade/intermittent/associated with chills
and rigor
History of altered sensorium since 1 day
History of vomiting for 1 day -4 to 5 episodes /not blood stained
Non bilousnon projectile
PAST HISTORY :
K/C/O Miliary tuberculosis (completed treatment)
14
15.
On Admission
Patient drowsy/not oriented/respond occasionally to oral
commands
Hydration fair/pallor
present SYSTEMIC
EXAMINATION: CVS:S1S2 +
RS: BILATERAL AIR ENTRY+
CNS: Drowsy /disoriented
Bilateral pupils equally reactive to
light Bilateral plantar FLEXOR
No neck stiffness
BP 120/80mmhg
PR 96/min
Spo2 99% in RA
15
MRI BRAIN -CONTRAST:
EARLYOBSTRUCTIVE HYDROCEPHALUS WITH DIFFUSE MENINGEAL
THICKENING IN BILATERAL TEMPORAL REGION
TO CONSIDER MENINGITIS Serum osmolality 264 mosm/l
Urine osmolality 310 mosm/l
Urine sodium 56 mEq/l
Urine potassium 16 mEq/l
TSH 1.7 mIU/ml
FT4 1.3 ng/dl
17
18.
Differential Diagnosis
- MILIARYTUBERCULOSIS / ?TB MENINGITIS
- SIADH
- HYDROCEPHALUS ASSOCIATED HYPONATREMIA
Hydrocephalus associated hyponatremia – increased pressure on hypothalamus
leads to release of ADH , which inturn causes hyponatremia
Treating the underlying problem is main stay of treatment
18
19.
Case no.5
A 50/fMrs.Vijayalashmi came with
Complaints of lethargy,irritability for last 1week History of vomiting present
for last 2 days
Non bilous,non projectile,contains food particles / Not blood stained
No history of fever
Past history:
K/c/o seizure disorder for past 4 years on T.phenytoin 100mg 1-0-2,
T.phenobarbitone 30mg 0-0-1
19
20.
On examination
Patient awake,responds to oral commands
Afebrile ,not dyspneic,hydration fair ,no pallor,no pedal edema
Systemic examination:
CVS:S1S2 +
RS: BILATERAL AIR ENTRY+
P/A:SOFT
CNS: Bilateral pupils equally reactive to light
Bilateral plantar FLEXOR
No neck stiffness
20
Serum calcium: 10.6mg
Serumcortisol: 2.2mcg/dl(2.9 – 17.3)
Performing the ACTH stimulation test requires measurement of serum cortisol in
early am, then the patient is given 250 mcg of cosyntropin IV. Serum cortisol is
measured 30 minutes and 60 minutes later. A serum cortisol level > 18-20 mcg/dl
is a normal response
MRI brain -Normal study
23
HYPOCORTISOLISM - HYPONATREMIA
•Due to increase in antidiuretic hormone (ADH) level resulting in retention of free
water
• Cortisol deficiency also leads to an increase in cortisol releasing hormone (CRH)
from hypothalamus which is an ADH secretagogue.
• Cortisol has negative feedback on CRH and ACTH
• Cotisol also causes direct suppression of ADH secretion
• Decreased cortisol level result in increased ADH level – free water retention and
hyponatremia
25
26.
Hyponatremia
Hyponatremia is definedas a plasma Na+ concentration <135 mEq/L
Mild hyponatremia: serum Na 130-134 mEq/l
Moderate hyponatremia: serum Na 125-129 mEq/l
Severe or profound hyponatremia: serum Na <125 mEq/l
Acute hyponatremia - < 48 h in duration
Chronic hyponatremia - >48 h in duration
26
27.
Pseudohyponatremia
Pseudohyponatremia is associatedwith severe hyperlipidemia or hyperproteinemia
It usually does not occur until the plasma lipid levels rise above 1,500 mg/dL or the plasma
protein levels rise above 12–15 g/dL
plasma osmolality, which will be normal in pseudohyponatremia, and reduced in “true” or
hypotonic hyponatremia.
Clinical presentation - hyponatremia
Mild -Headache, irritability,altered mood , hiccups
Moderate-Nausea,confusion, disorientation,altered mental status,unstable gait
Severe- Vomiting, seizure, Respiratory distress and coma
27
HYPOTONIC HYPONATREMIA
ADH isalso released in response to nonosmotic factors like a decrease in
blood pressure (via baroreceptors) or “physiological stress”
When nonosmotic stimuli for ADH release are active, ADH release persists
despite a plasma [Na] ≤ 135 mEq/L,the resulting water reabsorption in the kidneys
aggravates the hyponatremia.
Nonosmotic or “inappropriate” release of ADH is an important factor in the
development of severe and sustained hyponatremia.
29
SIADH CRITERIA -DIAGNOSTIC CRITERIA
ESSENTIAL CRITERIA
• Euvolemia
• Serum osmolality <275mosm/kg
• Urine osmolality >100 mosm/kg
• Urine Na+ >30mmol/L
• No recent use of diuretics
• Normal adrenal,renal,thyroid function
SUPPLEMENTARY CRITERIA:
• serum uricacid<4mg/dl
• Serum urea<21.6mg/dl
• Failure to correct hyponatremia after
0.9% saline infusion
• Fractional sodium excretion >0.5%
• Fractional urea excretion>55%
• Fractional uric acid excretion>12%
• Correction of hyponatremia through
fluid correction
31
32.
Cerebral salt wasting
•CSW– BNP (circulating factors) and sympathetic nervous dysfunction
• CSW are dehydrated which is a distinguishing feature from patients with SIADH
who are euvolemic.CSW is seen in patients with CNS disease especially several
days after subarachnoid hemorrhage
• Clinical findings – Hypovolemia – hypotension, tachycardia, dry mucous
membrane , postural hypotension
Dehydration – elevated hematocrit
Negative fluid balance – input output chat
• CSW is characterized by hyponatremia, serum hypo osmolality, urine
osmolality
>100-300 mOsm/kg H2O, urine Na > 40 mEq/l.
• Treatment – Treat the underlying cause and isotonic saline for mild to moderate
32
33.
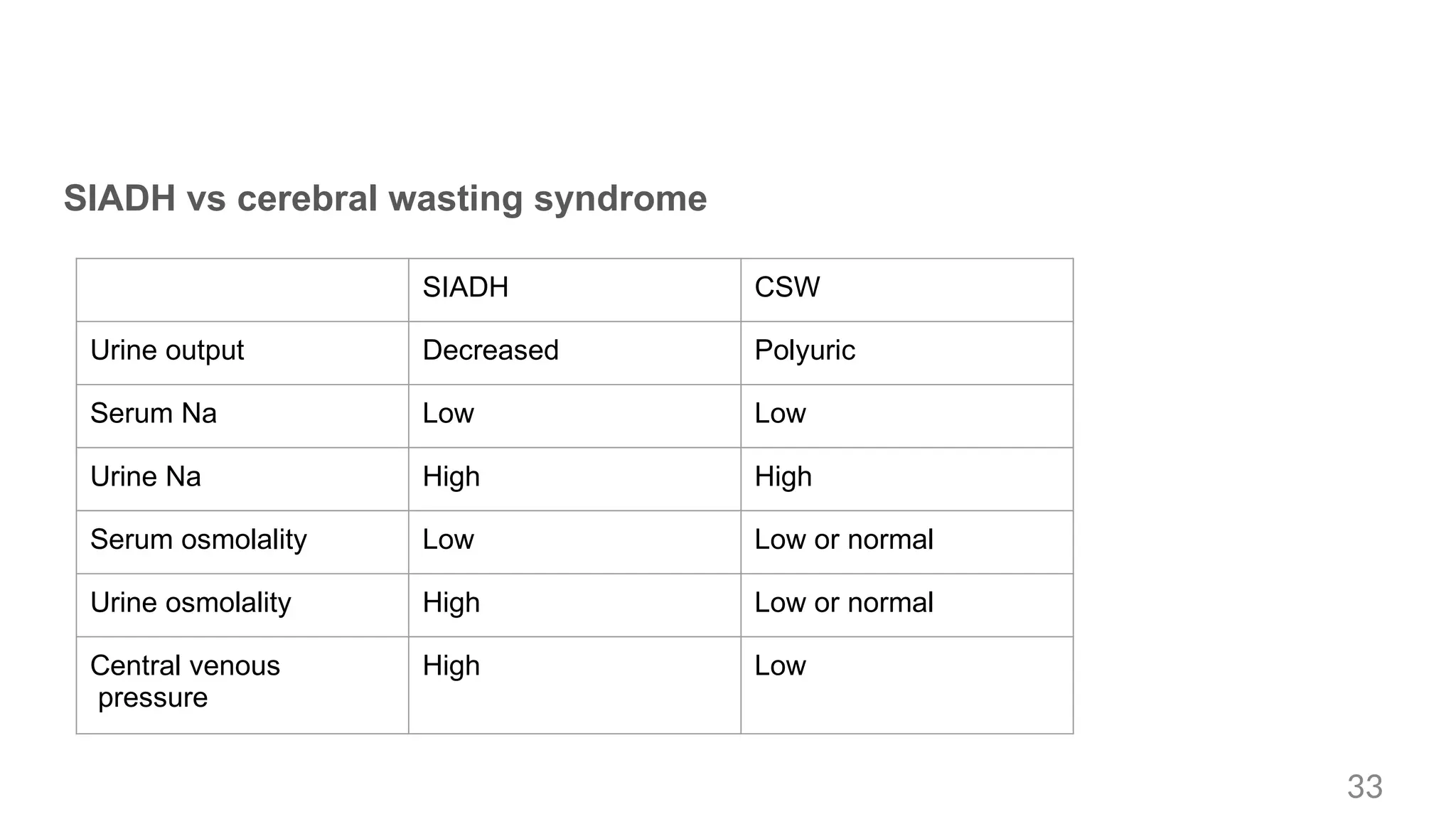
SIADH vs cerebralwasting syndrome
SIADH CSW
Urine output Decreased Polyuric
Serum Na Low Low
Urine Na High High
Serum osmolality Low Low or normal
Urine osmolality High Low or normal
Central venous
pressure
High Low
33
34.
Treatment of hyponatremiawith severe symptoms
First hour:
150ml 3% hypertonic over
20 mins IV
Recheck after 20 mins
Can be repeated twice or
5mmol/l increase in serum
sodium is achieved.
If symptoms improved No improvement
Stop infusion Continue IV infusion-
1mmol/l increase
Limit the increase in serum
sodium concentration to
total of 10 mmol/ l during
first 24 hours
Stop- symptoms
improve,increases to
10mmol/l, serum sodium
reaches 130mmol/l
8mmol/l during every 24
hour until serum sodium
concentration reaches
130mmol/l
4th hourly monitor -iv
infusion
6th and 12th h and daily
afterwards
34
35.
Moderate severe symptoms
•150ml 3% hypertonic over 20 mins IV
• Increase of 5mmol/l per 24hour in serum sodium concentration
• Limit the increase in serum sodium concentration to total of 10 mmol/ l during first
24 hours
• 8mmol/l during every 24 hour until serum sodium concentration reaches
130mmol/l 1,6 and 12th hourly
35
36.
Without severe ormoderately severe symptoms
Acute Chronic
• If a acute decrease exceeds 10mmol/l
• Single IV infusion of 150ml 3% hypertonic
over 20 mins
• Monitor serum sodium after 4th hour
• Treat cause
• Avoid increase in serum sodium
concentration to >10 mmol/ l
during first 24 hours and >8mmol/l
during every 24 hour
• Monitor 6th hourly
36
37.
osmotic demyelination syndrome(ODS)
• Quick correction especially >12 mEq/ 24 h might lead to osmotic
demyelination syndrome (ODS)
• This disorder is encountered more often after rapid correction of chronic hyponatremia
rather than acute hyponatremia. It is a rare but serious condition that occur 2-6 days
after rapid correction of sodium
• It manifests with dysarthria, dysphagia, behavioral disturbances, paraplegia
or quadriplegia, coma and seizures
• The diagnosis is made with MRI.
• Risk factors for ODS
include sodium level <120 mEq/l, alcoholism, liver disease and malnutrition
37
38.
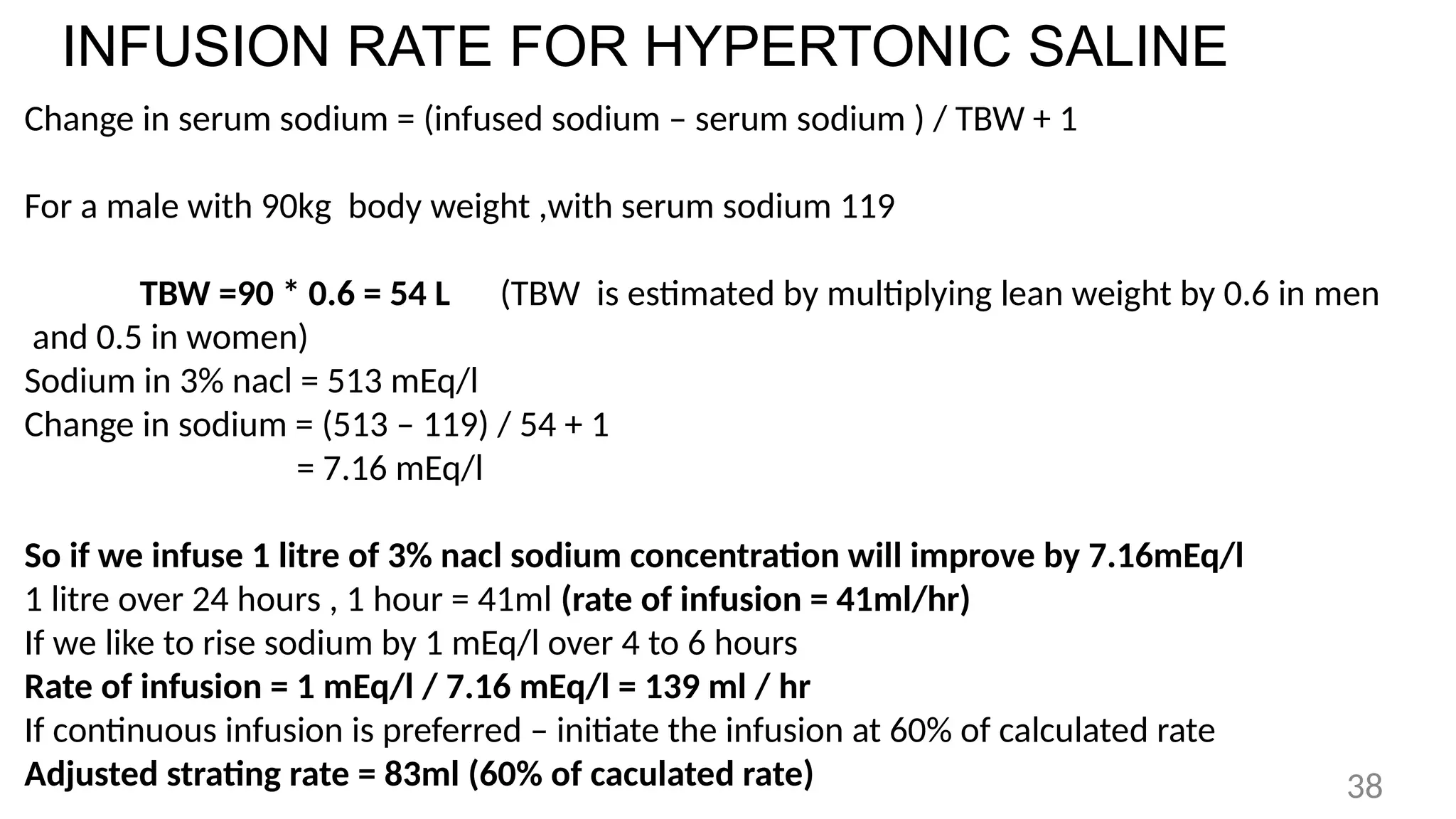
INFUSION RATE FORHYPERTONIC SALINE
Change in serum sodium = (infused sodium – serum sodium ) / TBW + 1
For a male with 90kg body weight ,with serum sodium 119
TBW =90 * 0.6 = 54 L (TBW is estimated by multiplying lean weight by 0.6 in men
and 0.5 in women)
Sodium in 3% nacl = 513 mEq/l
Change in sodium = (513 – 119) / 54 + 1
= 7.16 mEq/l
So if we infuse 1 litre of 3% nacl sodium concentration will improve by 7.16mEq/l
1 litre over 24 hours , 1 hour = 41ml (rate of infusion = 41ml/hr)
If we like to rise sodium by 1 mEq/l over 4 to 6 hours
Rate of infusion = 1 mEq/l / 7.16 mEq/l = 139 ml / hr
If continuous infusion is preferred – initiate the infusion at 60% of calculated rate
Adjusted strating rate = 83ml (60% of caculated rate) 38
39.
INFUSION RATE FORHYPERTONIC SALINE
Multiplying the patients body weight (in kg) by the desired rate of increase in
plasma [Na]
For example,
Patient weighs 70 kg
Desired rate of rise in plasma [Na] is 0.5 mEq/L per hour,
the initial infusion rate of hypertonic saline is 70 × 0.5 = 35 mL/hr.
The plasma [Na] is monitored periodically to determine when the target plasma
[Na] (120 mEq/L) is achieved
Paul L marino 39
40.
Asymptomatic hyponatremia -Treatment
Hypovolemic hyponatremia - Isotonic saline can be used to restore the
intravascular volume
Hypervolemic hyponatremia - Definitive treatment requires management of the
underlying condition and fluid restriction.
Increasing sodium in the patient’s diet will worsen his CHF symptoms
SIADH - The standard first-line therapy is water restriction and correction of any
contributing factors
40
41.
PHARMACOLOGICAL
Demeclocycline -
Tetracycline derivativethat blocks effects of ADH in renal tubules. SIADH
and chronic hyponatremia who do not tolerate fluid restriction Dose is 600–
1200 mg daily in divided doses,Nephrotoxic.
Vasopressin Antagonists:contraindicated in hypovolemic hyponatremia
CONIVAPTAN: loading dose of 20 mg IV, followed by a continuous infusion of 40 mg/day
for 96 hours.
6–7 mEq/L increase in plasma [Na] in the first 24 hours of drug infusion,
maintained for the 96-hour infusion period.
Tolvaptan- starting at a dose of 15 mg once daily, and increasing the dose, if
necessary, to a maximum of 60 mg daily , not exceeding 30 days
Side effects : liver toxicity,dry mouth,thirst
41



![HYPEROSMOLAR HYPONATREMIA
• Osmotically active solutes other than sodium accumulates in ECF , drawing water
into ECF and diluting the sodium content.
CAUSES :Hyperglycemia , post transurethral resection of prostate syndrome –
transient hyponatremia – bladder irrigation –glycine, sorbitol, mannitol.
Hyponatremia associated with severe hyperglycemia is not considered
pseudohyponatremia. It is the result of sodium dilution due to water shift from the
intracellular compartment
serum sodium decreases by about 1.6 mEq/l for every 100 mg/dl of glucose
above the normal range which is around 100 mg/dl
Corrected sodium = measured sodium + [1.6 x (measured glucose -100/100)]
5](https://image.slidesharecdn.com/hyponatremiacasereport-250324045617-d2f0db3c/75/HYPONATREMIA-CASE-REPORT-pptx-in-our-college-5-2048.jpg)














![HYPOTONIC HYPONATREMIA
ADH is also released in response to nonosmotic factors like a decrease in
blood pressure (via baroreceptors) or “physiological stress”
When nonosmotic stimuli for ADH release are active, ADH release persists
despite a plasma [Na] ≤ 135 mEq/L,the resulting water reabsorption in the kidneys
aggravates the hyponatremia.
Nonosmotic or “inappropriate” release of ADH is an important factor in the
development of severe and sustained hyponatremia.
29](https://image.slidesharecdn.com/hyponatremiacasereport-250324045617-d2f0db3c/75/HYPONATREMIA-CASE-REPORT-pptx-in-our-college-29-2048.jpg)




![INFUSION RATE FOR HYPERTONIC SALINE
Multiplying the patients body weight (in kg) by the desired rate of increase in
plasma [Na]
For example,
Patient weighs 70 kg
Desired rate of rise in plasma [Na] is 0.5 mEq/L per hour,
the initial infusion rate of hypertonic saline is 70 × 0.5 = 35 mL/hr.
The plasma [Na] is monitored periodically to determine when the target plasma
[Na] (120 mEq/L) is achieved
Paul L marino 39](https://image.slidesharecdn.com/hyponatremiacasereport-250324045617-d2f0db3c/75/HYPONATREMIA-CASE-REPORT-pptx-in-our-college-39-2048.jpg)

![PHARMACOLOGICAL
Demeclocycline -
Tetracycline derivative that blocks effects of ADH in renal tubules. SIADH
and chronic hyponatremia who do not tolerate fluid restriction Dose is 600–
1200 mg daily in divided doses,Nephrotoxic.
Vasopressin Antagonists:contraindicated in hypovolemic hyponatremia
CONIVAPTAN: loading dose of 20 mg IV, followed by a continuous infusion of 40 mg/day
for 96 hours.
6–7 mEq/L increase in plasma [Na] in the first 24 hours of drug infusion,
maintained for the 96-hour infusion period.
Tolvaptan- starting at a dose of 15 mg once daily, and increasing the dose, if
necessary, to a maximum of 60 mg daily , not exceeding 30 days
Side effects : liver toxicity,dry mouth,thirst
41](https://image.slidesharecdn.com/hyponatremiacasereport-250324045617-d2f0db3c/75/HYPONATREMIA-CASE-REPORT-pptx-in-our-college-41-2048.jpg)





































































