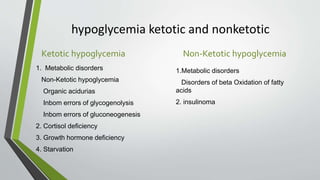
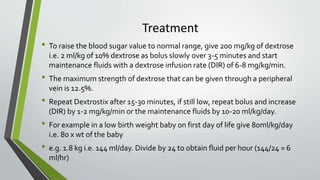
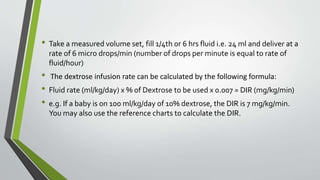
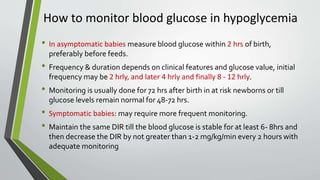
This document discusses hypoglycemia in neonates. It defines neonatal hypoglycemia as a plasma glucose level below 30 mg/dL in the first 24 hours of life or below 45 mg/dL thereafter. It identifies factors that increase hypoglycemia risk, such as low birth weight, prematurity, and maternal diabetes. Symptoms are nonspecific but include poor feeding, temperature instability, and central nervous system issues. Treatment involves glucose boluses and maintenance with intravenous dextrose infusions. Resistant or persistent hypoglycemia may require higher infusion rates, hydrocortisone, glucagon, or other drugs. Careful glucose monitoring is important to prevent neurological complications.