1) Preoperative hypertension is common and increases the risk of perioperative complications, however well-controlled hypertension may not need surgery postponement.
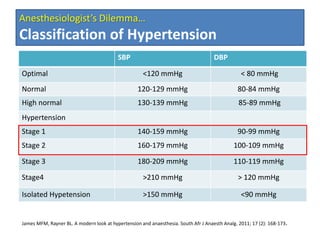
2) Isolated systolic hypertension over 180 mmHg and high pulse pressure over 80 mmHg are associated with increased risk and reasonable to postpone surgery.
3) Left ventricular hypertrophy and diastolic dysfunction from long-standing hypertension increase perioperative risk and require careful fluid management during surgery.