This study aimed to test a motivational interpretation of placebo effects using two different placebo therapies: flower essences and gratitude therapy. The motivational interpretation is that rituals consistent with self-actualizing goals have a nonspecific therapeutic benefit beyond expectations. Study 1 found that trait spirituality predicted perceived improvement from flower essences, independently of optimism and expectations. Study 2 found that trait gratitude predicted perceived sleep improvement from gratitude therapy, independently of expectations. These findings suggest that engagement with positive, therapeutic rituals, beyond expectations, determines the extent of the placebo response.
![Journal of Psychosomatic Research 62 (2007) 331 – 340
Dispositional predictors of placebo responding: A motivational
interpretation of flower essence and gratitude therapy
Michael E. Hyland4, Ben Whalley, Adam W.A. Geraghty
School of Psychology, University of Plymouth, PL48AA Plymouth, United Kingdom
Received 26 July 2006; received in revised form 11 October 2006; accepted 11 October 2006
Abstract
Objectives: The aim of this study was to test a motivational spirituality, and expectancy). Results: Study 1 confirmed previous
interpretation of placebo responding using two different types of research: Trait spirituality predicted perceived improvement. This
placebo therapy, one using flower essences and the other a improvement was independent of optimism ( Pb.001), cannot be
nonspecific psychological therapy. The motivational concordance explained by acquiescence or social desirability, and was inde-
interpretation is that therapeutic rituals that are consistent with self- pendent of a highly conservative test of expectancy ( P=.02). In
defining or self-actualizing goals have a nonspecific therapeutic Study 2, trait gratitude predicted perceived sleep improvement
benefit independently of expectancy. Methods: Study 1 was a independently of expectancy ( P=.01): Spirituality did not correlate
replication of an earlier flower essence outcome study but with with improvement. Conclusions: These data suggest that in
additional outcome and predictor variables: 167 people completed addition to expectations, degree of engagement in a positive,
questionnaires in return for free flower essence treatment. Predictor therapeutic ritual determines the extent of the placebo response.
variables consisted of two measures of spirituality, optimism, The placebo response depends in part on the interaction (i.e., the
expectancy, and attitudes and beliefs to complementary medicine. degree of concordance) between the type of therapy and the par-
Outcome was assessed after 3 weeks. In Study 2, 90 people took ticipant’s personality: Dispositional predictors vary with the type of
part in bgratitude therapyQ for improved sleep quality over one placebo therapy.
night in return for questionnaire completion (trait gratitude, D 2007 Elsevier Inc. All rights reserved.
Keywords: Placebo responder; Disposition; Personality; Motivation; Interaction; Positive psychology
Introduction an understanding of the dispositional predictors of placebo
responding suggests the existence of a motivational mecha-
In medicine, the word placebo refers to a biologically nism that is a nonspecific feature of all therapeutic rituals.
inactive treatment [1,2], typically a psychological mechanism
having nonspecific effects [3]. The use of the term placebo in
psychology includes the idea that, additionally, the placebo is The conventional perspective
an inactive psychological procedure [4]. The psychologists’
use of the term placebo creates problems in psychotherapy There is consensus that at least two mechanisms underlie
because many authors believe that nonspecific processes are the placebo response [7]. Response expectancy theory
important [5], and, in the case of the contextual model of suggests that the body responds in ways that are consistent
psychotherapy, that nonspecific mechanisms are the only with (conscious) expectations. Conditioning theory suggests
active processes [6]. The purpose of this paper is to show that that active treatments are unconditioned stimuli; the delivery
technique of the active treatment becomes a conditioned
4 Corresponding author. School of Psychology, University of Ply-
stimulus after repeated administration, so that the delivery
mouth, PL48AA Plymouth, United Kingdom. technique, or similar techniques, acquires therapeutic proper-
E-mail address: mhyland@plymouth.ac.uk (M.E. Hyland). ties similar to the active treatment. Although conditioning
0022-3999/07/$ – see front matter D 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.jpsychores.2006.10.006](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-1-2048.jpg)
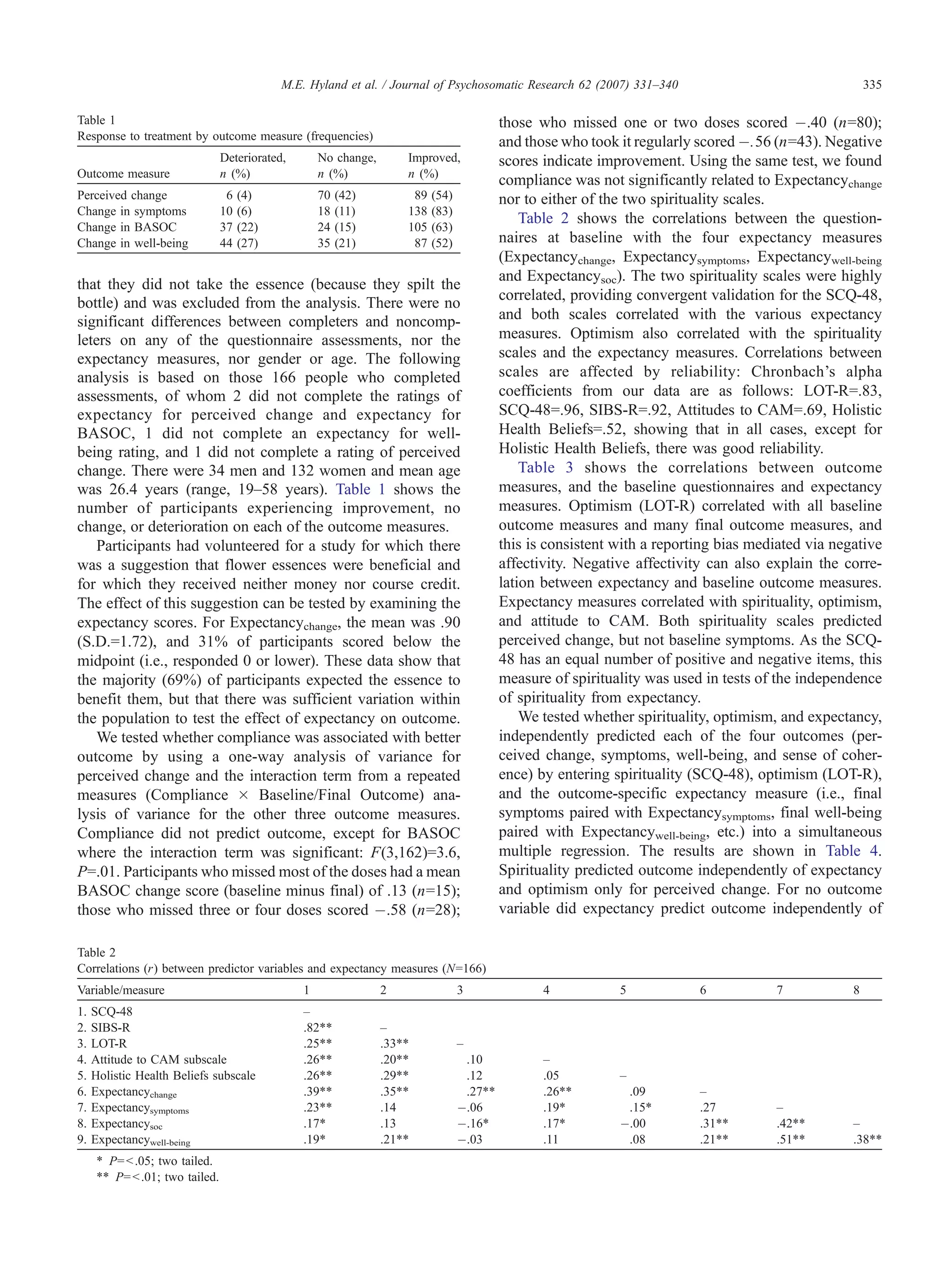
![332 M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340
can add to expectancy [7], it has been suggested that expec- and staff were offered free flower essences in return for
tancy is the more important mechanism because placebos completed questionnaires and evaluation. Expectancy, absorp-
can occur without any prior conditioning or experience of the tion, and spirituality were assessed at baseline, and perceived
active treatment, and conditioned placebos have been shown change was measured after 4 weeks. Expectancy, absorption,
to be mediated by expectancy [8,9]. and spirituality all correlated with outcome; spirituality but not
Although there is consensus over the mechanisms under- absorption predicted outcome independently of expectancy.
lying the placebo, there is less consensus on the personality These three studies all suggest that there may be some other
predictors of the placebo response. The majority view is that mechanism than expectancy underlying the placebo response,
there is no such thing as a placebo-responding personality particularly in real-life contexts where people are actively
[10,11]; that is, placebo response cannot be predicted from seeking treatment for their health problems.
dispositional variables. This view is based not on the absence
of correlations—many have been reported—but on reviews
showing that results are often inconsistent. The minority view Non-expectancy-mediated placebo mechanisms
is that there is sufficient consistency to identify one or more
personality predictors, and two that have been cited are Two different, non-expectancy-mediated hypotheses can
acquiescence [12] and optimism [13]. Both acquiescence and explain placebo effects in therapeutic contexts. An early
optimism fit within an expectancy model of placebo placebo hypothesis was based on motivation: The health
responding. People high in acquiescence are more likely to striving hypothesis suggests that people are more likely to
agree with a suggestion from an external source and so should get better when they are motivated to get well, compared
be more likely to expect a treatment to be effective when told with those less motivated to get well. There is some
so; people high in optimism are likely to make an optimistic evidence that motivation enhances placebo responding [29],
judgment about a treatment and so are more likely to expect and the health striving hypothesis is also consistent with the
the treatment to have a good effect when told so. Thus, finding that compliance in the placebo arm of a randomized
both acquiescence and optimism could be considered mo- drug trial is associated with better outcome—presumably
derators of the expectancy mechanism. because people who are more motivated to get better
comply more with their treatment [30,31].
An alternative motivational hypothesis is derived here
Evidence for non-expectancy-mediated mechanisms from a combination of two ideas. First, several well-
established motivational theories suggest that failure to
Complementary and alternative medicine (CAM) com- achieve important, high-level, self-actualizing, or self-
prises a diverse group of therapies that fall outside the remit defining goals has negative mental consequences. By
of conventional medicine and that are widely used by the contrast, attaining these high-level, self-actualizing, or
general public [14–16]. The underlying mechanisms of self-defining goals leads to greater well-being [32–38].
CAM are controversial—which is, in part, why they fall Self-actualization refers to the goal to become the bperson
outside conventional medicine. Although the evidence for you really are,Q rather than achieve socially defined goals, so
specific components is mixed and researchers hold a variety there is an underlying assumption that what is bgoodQ for
of views, there is general acceptance by all parties that one person may not be so for another. Specifically, the self-
psychological factors are important. concordance model [35] suggests that people put more
Meta-analyses of double-blind placebo controlled trials of effort into, and gain more satisfaction from, the attainment
homeopathy show large placebo effects that add a methodo- of self-defining goals. Second, we use an idea from the
logical challenge to the demonstration of any additional contextual model of psychotherapy [6]: A common feature
specific effect [17–19]. However, a large (N=202) double of all psychotherapies, as well as traditional healing rituals,
blind, randomized, controlled trial of a homeopathic is that the patient believes in and engages in a health-
preparation for asthma [20] failed to find any correlation promoting ritual, although the ritual may be based on a myth
between a surrogate measure of expectancy, attitude to that is not btrueQ [39]. The motivational concordance
CAM, and the improvements in physiological or psycho- hypothesis combines these two ideas: Engaging in health-
logical outcome [21]. Similarly meta-analyses of sham vs. promoting rituals that enhance self-defining or self-actualiz-
real acupuncture suggest a large placebo effect [22–24], but a ing goals provides better outcomes when compared to
large (N=239) open study found that there was a non- health-promoting rituals that are not. Or to put it from an
significantly better outcome amongst those who did not existential perspective, receiving therapy that is consistent
believe in acupuncture [25]. with the breal youQ [40] is associated with therapeutic gain,
The above two studies did not investigate expectancy irrespective of gain mediated via expectancy processes. This
directly. Flower essence therapy is related to homeopathy and motivational hypothesis differs from the contextual model
the only two double-blind placebo-controlled trials of this of psychotherapy in suggesting that the therapist is not an
therapy have failed to find a difference between placebo and essential part of a therapeutic ritual. Taking part in rituals
verum [26,27]. In an open study [28], 116 university students that are concordant with self-actualizing or self-defining](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-2-2048.jpg)
![M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340 333
goals has a therapeutic effect alongside other mechanisms, essence in return for questionnaire completion. The adver-
such as response expectancy. tisements informed participants about a commercial Web
Why do people show a better placebo response to flower site on flower essences. They were told that the effect of
essences if they are high in spirituality? Edward Bach, the flower essences was purported to have a therapeutic effect,
inventor of flower essences, was a homeopath who also that this claim was controversial, and that the researchers
believed that illness had a spiritual basis and could be cured were investigating flower essences. Participants were
spiritually [41]. Thus, flower essences, like some other neither paid nor received course credit for taking part.
CAMs, appear to have the psychological context of a
spiritually oriented therapy, or at least can be interpreted as Predictor questionnaire assessments
a spiritually oriented therapy. People who score highly on a We used two measures of spirituality. The 22-item
spirituality scale are more likely to use CAM [42]. Since Spiritual Involvement and Beliefs Scale—Revised (SIBS-
taking flower essences is a ritual, one possible explanation is R; Hatch, personal communication, 2001) is the revised
that those high in spirituality strive more, and so bdo the version of an earlier 39-item scale [44] that purports to
ritualQ better, than those low in spirituality. Because the measure spirituality in contrast to religiosity. Participants
ritual is more congruent with their self-defining goals, respond to each item on a 7-point scale, and high scores
spiritual people gain more benefit from flower essence indicate greater spirituality. Although there are more
therapy. In more general terms, the motivational concord- positive than negative items, the authors report that the
ance hypothesis suggests that a good placebo is one that scale is uncorrelated with social desirability (Hatch,
matches the context of the therapy to the motivational personal communication, 2006). We included this scale
system of the client, so that the behavioral ritual of the because it had been used in an earlier study [28].
therapy is concordant with the client’s motivations. The The second spirituality measure, the 48-item Spiritual
concordance between the ritual and motivation does not just Connection Questionnaire (SCQ-48), was specially designed
provide expectancies for positive outcome but has an for this study, as no other spirituality scale has equal numbers
independent effect on outcome. of positive and negative items. The scale was based on the
Hunglemann et al. [45] definition of spirituality as a bsense of
interconnectedness between self, others, nature and Ultimate
Study 1 which exists throughout and beyond time and spaceQ (p. 152).
Scale items cover the experience of a bsense of connectionQ in
Correlations between personality and placebo outcome the following domains: with the universe, e.g., bI do not feel
are notoriously fickle. The aim of Study 1 was to replicate connected to the universe in any spiritual wayQ; with people,
the earlier flower essence study [28], but using a larger bThere is something of the cosmos that binds all people
sample size and some additional measures. togetherQ; with nature, bI never feel any special connection
First, we used an additional measure of spirituality that has with a part of nature such as a flowerQ; and with places, bI
equal numbers of positive and negative items. In the earlier sometimes experience joy just from being in a beautiful
study, the spirituality scale had more positive items, so the place.Q Thus, the SCQ-48 is a scale measuring the experience
spirituality–outcome correlation could have been due to of spirituality that is related to a sense of connection.
acquiescence bias. Second, we measured optimism because Participants respond to each item on a 7-point scale, and
optimism has been reported elsewhere as a predictor of high scores indicate greater spirituality. Research reported
placebo outcome [43] and because the spirituality–outcome elsewhere [46] shows the scale to be unidimensional, with the
correlation may be mediated via optimism. Third, we used first factor accounting for 48% of the total variance; that the
additional outcome measures, linked to additional measures scale fails to correlate (r=.03) with the Marlow–Crowne scale
of expectancy. The additional expectancy measures provide a (social desirability); and that it has high internal consistency
stricter test of the independence of the spirituality–outcome (a=.97) and retest reliability (r=.99).
link from expectancy. The additional outcome measures Optimism was measured using the 10-item Life Ori-
allow us to examine the nonspecific effects of the treatment entation Test—Revised (LOT-R) [47], which contains six
(i.e., benefits beyond those for which the treatment is taken) scored items (three positively worded, three negatively
and also allow a check on whether the correlation with worded) and four filler items; participants respond to each
spirituality occurs with actual symptom change rather than item on a 5-point scale, and higher scores indicate greater
perceived change. optimism. Optimism has been found to predict placebo
responding [43] and correlates with neuroticism.
Method The 11-item Holistic Complementary and Alternative
Medicine Questionnaire (HCAMQ) [48] has two subscales:
Recruitment Attitudes to Complementary Medicine, and Holistic Health
Participants were recruited through advertisements Beliefs. The two subscales are based on evidence that the
posted throughout the university and at a neighboring art parent scale has two distinct but correlated factors.
college. The advertisements offered a free bottle of flower Participants respond on a 7-point scale, and high scores](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-3-2048.jpg)
![334 M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340
indicate greater positivity to CAM and more holistic health (Expectancysoc) was scored by subtracting the expected
beliefs. Both subscales correlate with expectancy of out- BASOC values from the baseline score; higher scores indicate
come with flower essences [28]. greater expectancy for improvement in sense of coherence.
Outcome and expectancy measures Compliance
To measure expectancy for perceived change (Expect- After the final assessment, participants were asked to
ancychange) participants were asked: bAt this point in time, indicate which statement best applied: I took it regularly (4),
do you expect the flower essence to help you?Q Participants I missed doses 1 or 2 days per week (3), I missed doses 3 or
were asked to bcircle the number that describes your 4 days per week (2), I missed most of the doses (1), or I did
opinionQ on an 8-point scale ranging from Yes, I definitely not take the essence (0).
think it will help (8), to I think it very unlikely it will help me
(1). Perceived change was assessed by e-mail. The e-mail Procedure
stated, bThank you for taking part in our experiment. You On arrival at the advertised drop-in session, participants
chose [name of essence] for [original symptoms].Q Partic- gave written informed consent and were presented with
ipants were then asked, bBelow, you will see a perceived the list of 38 Bach flower essences and descriptions of the
change scale. Please make a note of the number on the scale conditions for which each essence can be used. Each of the 38
that you think best illustrates your perceived change.Q flower essences purports to benefit particular psychological
Responses were made on a 7-point Likert-type scale problems. For example, if you are bcritical and intolerant of
(À3 to +3) where the word worse was positioned near othersQ then Beech is recommended; if you bare inflexible,
À3 and better near +3. setting yourself very high standardsQ then Rock Water should
Whereas Hyland et al. [28] used only perceived change as be used; and if bimpatient or easily irritated,Q then Impatiens
an outcome measure, in this study we measured symptoms is used. An essence is (typically) made by floating a flower in
before and after treatment. At baseline participants rated the spring water in a clear glass bowl in bright sunlight for 3
two symptoms for which they had initially selected the flower hours and preserving this water in a solution of water and
essence, using two, 7-point scales; the end points were brandy (40% water, 60% brandy). A few drops of this
labeled no problem (0) and as bad as it could be (6). bmother essenceQ are then added to 10-ml bottles of water and
Participants also rated the same symptoms in terms of how brandy (again 40% and 60%, respectively) to form bstockQ
they expected the symptom to be after 3 weeks of treatment essence, which was provided by the manufacturer.
with flower essences (with the first rating in sight). After Participants were told they could choose up to two
3 weeks, they were asked, via e-mail, to rate their symptoms essences. In addition to indicating their choice of essence,
again, but without sight of the original ratings. Baseline and they completed the questionnaire pack (SQC-48, SIBS-R,
final symptom scores were obtained by adding the values for LOT-R, and HCAMQ).
the two symptoms at baseline and final assessment, respec- Participants were then asked to provide baseline outcome
tively. Expectancies for changes in symptoms (Expect- ratings (symptoms, well-being, and sense of coherence), and
ancysymptoms) were obtained by subtracting the two values also to provide ratings on the same scales for where they
for expected symptoms from the baseline symptom score; expected to be after the flower essence treatment (these were
higher values indicate an expectancy of better outcome. used to calculate expectancy scores).
Advocates of CAM suggest that their treatments have Participants were given their chosen essences, made by
effects beyond the symptoms for which patients seek placing two drops of stock essence in a 10-ml bottle of
assistance [49]. We therefore included two other outcome brandy (60%) and spring water (40%) solution (i.e., no
measures, neither of which was directly related to the deception was involved). They were thanked and reminded
intended treatment. Well-being was measured at baseline to expect the e-mail follow-up to be sent 3 weeks later. E-
with a 7-point scale of well-being: Participants were asked to mail data collection has been shown to be valid and
bRate your general feeling of well-being during the last equivalent to traditional methods [51]. Participants who
week.Q Responses were taken on a scale that ranged from as did not reply to the follow-up were sent reminder e-mails
good as it could be (0) to as bad as it could be (6). Participants one week later (note: a small minority of participants asked
also rated where they expected to be after 3 weeks using to give their replies via the telephone). The follow-up and
the same scale. Final well-being was measured (via e-mail) reminder e-mails asked for ratings of perceived change, the
using the same scale at 3 weeks. Expectancy for well-being two symptoms, well-being, the three sense of coherence
(Expectancywell-being) was scored by subtracting the expected items, and a response to the compliance question.
well-being score from the baseline score. Sense of coherence
was assessed with the 3-item version of the Brief Assessment Results
of Sense of Coherence (BASOC) [50], where each item was
rated on a 5-point scale. Baseline and final BASOC scores Two hundred forty-three participants from the university
were the sum of the three scores at baseline and final and art college took part in the first part of the study, of whom
assessment, respectively. Expectancy for sense of coherence 167 completed follow-up assessments. One person indicated](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-4-2048.jpg)
![336 M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340
Table 3
Correlations (r) between outcome measures and predictors
Symptoms Well-being BASOC
Variable Perceived change Baseline Final (change) Baseline Final (change) Baseline Final (change)
SCQ-48 .2644 .07 À.09 (.14) .01 .09 (.06) .06 .04 (À.02)
SIBS-R .204 À.01 À.11 (.09) .01 .11 (.08) .12 .14 (.02)
LOT-R À.01 À.204 À.12 (À.04) .3744 .224 (À.11) .5244 .3244 (À.2044)
Attitude to CAM subscale .174 .254 À.01 (.2044) À.03 .10 (.10) À.01 .10 (.11)
Holistic Health Beliefs subscale À.00 .09 .08 (.00) À.03 À.05 (À.02) .02 À.09 (À.11)
Expectancychange .2144 .05 À.214 (.2344) .09 .15 (.05) .05 .10 (.05)
Expectancysymptoms .144 .4944 .02 (.3544) À.2544 À.08 (.13) À.174 b.01 (.174)
Expectancysoc .3044 .224 À.10 (.2644) À.2644 À.01 (.194) À.4844 À.13 (.3544)
Expectancywell-being .15 .234 b.01 (.1744) À.6844 À.10 (.4544) À.2544 À.04 (.2144)
4 P=b.05; two tailed.
44 P=b.01; two tailed.
spirituality and optimism. However, for perceived change, spirituality on perceived change is independent of expect-
there was a nonsignificant trend ( P=.07) suggesting the ancy and related variables, and spirituality does not interact
possibility of an independent effect of expectancy. Coupled with expectancy.
with the correlation of .21 between expectancy and
perceived change, we cannot rule out an independent Discussion: Study 1
contribution of expectancy on this outcome measure.
As spirituality predicted only perceived change, we We replicated the earlier finding (Hyland et al. [28]) that
carried out a more stringent test on this outcome variable. spirituality predicts perceived change of symptoms follow-
All four expectancy measures, plus Attitude to CAM and ing flower essence treatment, and, because we used a
Holistic Health Beliefs (i.e., the two HCAMQ subscales) spirituality scale with equal number of positive and negative
were entered into the first step of a hierarchical multiple items (SCQ-48), these new data suggest that the correlation
regression, R 2(6,156)=.115, P=b.01; with spirituality in the is not due to acquiescence bias. The correlation is unlikely
second step, DR 2=.03, P=.02. Thus, spirituality predicted to be due to social desirability, as the SCQ-48 is unrelated to
perceived change independently of all the other variables social desirability, and is unlikely to be mediated via
(b=.20). We tested whether there was an interaction between optimism, as optimism failed to predict change, although
expectancy and spirituality as predictors of perceived it did predict baseline symptom and other variables. These
change by entering the product term (Expectancychange  baseline correlations are to be expected as the LOT-R is
SCQ-48) in a third step of the multiple regression; there was highly correlated with trait neuroticism [47], and trait
no evidence of an interaction (b=À.09, P=.77). We tested affectivity affects symptom reporting [52]. Although sense
for other possible interactions (e.g., optimism and expect- of coherence and well-being increased after the flower
ancy) and none were significant. In sum, the effect of essence treatment, they were unrelated to spirituality, as was
Table 4
Simultaneous multiple regressions to test whether outcome is predicted independently by spirituality and expectancy
Dependent variable Predictor variables B S.E. b
Perceived change Expectancychange .04 .419 .15 ( P=.07)
LOT-R À.12 .09 À.11
SCQ-48 .21 .08 .234
Symptom final Symptom baseline .44 .10 .364
Expectancysymptoms À.14 .09 À.15
LOT-R À.04 .10 À.03
SCQ-48 À.08 .08 À.07
Well-being final Well-being baseline .19 .12 .19
Expectancywell-being .02 .13 .02
LOT-R .23 .15 .14
SCQ-48 .06 .11 .05
BASOC final BASOC baseline .51 .09 .524
Expectancysoc .16 .10 .13
LOT-R .07 .07 .08
SCQ-48 À.02 .05 .05
For perceived change, R 2(3,159)=.09, P=b.01; for symptom final, R 2(4,161) = .12, P=b.01; for well-being final, R 2(4,160)=.07, P=.01; and for BASOC final,
R 2(4,159)=.26, P=b.01.
4 P=b .01; two tailed.](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-6-2048.jpg)
![M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340 337
symptom change. There are several possible reasons for this Therapy to help your sleep?Q Participants were asked to
failure, one of which is that use of before and after measures bcircle the number that describes your opinionQ on an 8-point
increases the variance, and our study was underpowered in scale ranging from I think it very unlikely it will help me (1)
that regard. In addition, correlations between outcome and to Yes, I definitely expect it will help (8).
all predictors are reduced to the extent that outcome is The measure of change in perceived sleep quality was
affected by natural variation in symptoms over time. based on that used by Geers et al. [53]. The measure
The problem with the use of a physical therapy, such as consisted of five items measuring change in sleep quality.
flower essences, is that the psychological nature of therapy The items included bHow peaceful was your sleep last
is inferred. We have inferred the spirituality of flower night?Q and bHow would you rate your quality of sleep last
essences on the basis of the literature, not on the basis of night?.Q Items were rated on a 7-point scale ranging from
participant report. We have no way of telling from our data much worse than usual (1) to much the same as usual (4)
how flower essences were interpreted, and this is clearly a and much better than usual (7). These scores were totaled to
weakness in the interpretation we have provided for our create a bperceived sleep changeQ score.
data. An alternative way of testing the therapeutic ritual
hypothesis is to use a psychological therapy, where the Procedure
psychological nature of therapy is explicit in the therapy On arrival at the advertised drop-in sessions, partic-
itself. For Study 2, we invented a new therapy called ipants gave written informed consent and then completed
bgratitude sleep therapy.Q Our therapy was based on Geers the two questionnaires (GQ-6 and SCQ-48). Then, they
et al.’s [53] bplacebo sleep therapy,Q but we modified the were given an envelope containing a bgratitude sleep
instructions so that instead of asking participants to write therapyQ booklet, which contained instructions for the task,
down things that they had done, they were asked to write space in which to write things they felt grateful for, and
down things they were grateful for. Previous research has experimenter contact information. Participants were asked
shown that similar gratitude activities improve perceived to open the envelope and read the instructions, replace the
well-being [54,55]. If the therapeutic ritual hypothesis is booklet in the envelope, and then rate how much they
correct, then outcome to gratitude sleep therapy should expected the therapy to work. They were then asked to take
correlate with trait gratitude, but it should not correlate with the envelope home and complete the therapy that evening.
trait spirituality. In addition, participants were informed that their booklet
would not be collected by the experimenter and that their
notes would be seen by only them, allowing participants to
Study 2 express themselves without fear of others seeing their
writing. Participants were contacted by e-mail on the
Method following day and asked to complete the questions about
sleep quality.
Recruitment
Advertisements were placed around the university Results
campus offering those with sleep problems a free psycho-
logical treatment in return for questionnaire completion. Ninety-three people attended drop-in sessions, of whom
90 (37 men and 53 women) completed the follow-up
Questionnaires and Assessments assessment. Fifty-six percent were aged under 24 years,
The Gratitude Questionnaire—6 (GQ-6) is a six-item 25% were between 25 and 34 years. Amongst respondents,
scale developed to measure dispositional gratitude [55]. The 75% reported improvement, 9% reported no change, and 16%
scale features four positive items and two negative items, got worse. The mean value for Expectancy was 5.15
including bI have so much in my life to be grateful forQ and (S.D.=1.73); 27.5% scored at or below the midpoint of 4,
bI am grateful to a wide range of people.Q Participants indicating that they did not expect the therapy to be effective.
respond to items on a 7-point scale and high scores indicate Table 5 shows bivariate correlations for all the variables.
greater gratitude. Internal reliability for the six-item scale Spirituality (SCQ-48) and gratitude (GQ-6) were correlated,
was a=.72. The GQ-6 correlates with optimism and with consistent with previous research [55]. Gratitude and
spiritual transcendence [56], which includes the concept of expectancy correlated with outcome, but spirituality did
connectivity measured by the SCQ-48. not correlate with outcome. Using perceived sleep change as
Spirituality was measured by using the SCQ-48, that is, the dependent variable, we carried out a hierarchical
the scale used in Study 1. multiple regression to test the relative importance of our
Expectancy was measured by a single-item scale indicat- predictor variables. In Step 1, we entered Expectancy,
ing the extent to which they believed that their sleep would be R 2 (1,88)=.05, P=.03. In Step 2, we entered spirituality,
improved by the gratitude therapy. The scale was based on the which did not improve the model, DR 2=b.01, P=.93. In Step
Expectancychange measure used In Study 1. The question was 3, we entered gratitude, which improved the model,
bAt this point in time, do you expect the Gratitude Sleep DR 2=.07, P=b.01. Thus, gratitude (b=.28, P=b.01) and](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-7-2048.jpg)
![338 M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340
Table 5 pressor task. As these tasks are effective only when
Correlations between variables in Study 2
contextualized as pain relievers, this shows that they elicit a
Variable 1 2 3 meaning response. Participants’ reported level of absorption
1. Sleep outcome – with the task predicted outcome independently of expectancy,
2. GQ-6 .2744 – leading the authors to conclude that the task produced a non-
3. Expectancy .234 .08 –
expectancy-mediated effect. In these studies, like ours, there
4. SCQ-48 .08 .2744 .4244
is evidence that people gain more therapeutic benefit from a
4 P b.05.
44 P b.01.
ritual to the extent that the ritual is salient, and that this benefit
is independent of expectancy.
In addition, the importance of engagement with a ritual is
expectancy (b=.24, P=.03), but not spirituality (b=À.08, consistent with a study showing that self-help instructions
P=.48), predict perceived sleep change, with the final that are perceived as tailored to the needs of the person are
model, including gratitude and expectancy, accounting for more effective in producing change than nonpersonalized
12% of the variance in outcome. instructions [59]. Our interpretation of these data is that the
salience of a ritual is increased by its perceived relevance,
and personalizing increases perceived relevance.
Overall discussion Earlier reviews of the literature report inconsistency in the
placebo-responding personality or dispositional variables
How do placebos work in real-life contexts? Our research [10,11], and our results explain how this inconsistency can
suggests that two mechanisms are involved. One is the well- arise: The motivational context of the therapy affects the
established mechanism of response expectancy. The other is personality correlations. Studies 1 and 2 demonstrated the
a motivational mechanism where people gain therapeutic context specificity of personality–outcome correlations, but,
benefit by engaging in therapeutic rituals that are concordant additionally, were designed to rule out alternative explan-
with self-defining or self-actualizing goals. That is, when ations for personality–outcome correlations. There is no
people self-actualize as part of therapy, then this produces evidence that these correlations are mediated via optimism, or
therapeutic benefit through a motivational, non-expectancy- due to attitude towards therapy, or health beliefs. The
mediated pathway. disposition–outcome correlations are not due to acquiescence
In Study 1, we replicated an earlier finding that or social desirability because we used a spirituality scale that
spirituality predicted perceived change following treatment had equal numbers of positive and negative items and was
with flower essences. We reasoned that this occurred uncorrelated with social desirability. Finally, although we did
because the flower essences are conceptualized as a spiritual not have a nontreatment control, it is unlikely that the
therapy and spiritually oriented people bdo the ritualQ better, correlations with ritual-congruent dimensions would have
in the sense that they are more engaged with the ritual, and occurred as part of regression to the mean or natural history,
gain more satisfaction from taking flower essences. In Study because of the specificity of spirituality or gratitude to the
2, we found that dispositional gratitude but not spirituality particular type of therapy. Natural variation and regression
predicted perceived change following gratitude therapy. We must occur in both studies, and this variation will reduce the
reasoned that this was because people high in dispositional size of correlations between outcome and predictors. This
gratitude bdo the ritualQ better, in the sense that they find it reduction is exacerbated where the outcome measure is
easier to think about things to be grateful for, and find the unreliable, and where outcome is based on two (before and
process of doing gratitude more satisfying. after) measures. Therefore, in Study 1 the failure to find
Our interpretation is not definite at this stage. We do not independent personality predictors of symptom change, in
know whether motivational concordance leads to a greater contrast to perceived change, must be treated with caution.
focusing on positive symptoms, a tendency to ignore a Our research was motivated in part by some CAM studies
failure to benefit, or greater positivity, which translates into showing that expectancy is a poor predictor of outcome. In
therapeutic benefit. Our underlying assumption has been both our studies, expectancy was significantly correlated with
that fulfillment of self-actualizing goals, by engaging in the outcome, and the correlation coefficients were similar
therapeutic ritual, leads to general therapeutic benefit. We between the two studies (.21 for Study 1 and .23 for Study
cannot rule out the possibility that the effect is an effect 2). In Study 2, expectancy predicted outcome independently
only on symptom perception, although this would still be of personality, but in Study 1, the equivalent test just failed to
linked to motivation. reach significance ( P=.07). These results suggest that
Any motivational explanation for our findings leads to the expectancy does contribute to outcome, and possibly
corollary prediction that the degree of involvement with a independently, in both studies. However, it is clear that
therapeutic ritual contributes to outcome, and this prediction other mechanisms are involved. Our results do not bdisproveQ
has been confirmed elsewhere. In two earlier studies [57,58], the response expectancy explanation but instead show
participants were given distraction or imagery tasks that were that response expectancy is not the only mechanism.
presented as techniques for reducing pain perception in a cold However, it may be that in the richer context of a CAM](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-8-2048.jpg)
![M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340 339
treatment, expectancy becomes less important than in for Study 1. We thank Ainsworths, Healing Herbs, and the
laboratory analogue studies, so our results may not generalize Green Man Essence Company for help in providing
to laboratory-based studies where participants take part for materials used in Study 1 without charge or preconditions.
extrinsic reasons. Previous research has linked optimism with
placebo responding [43]. We found that optimism correlated
with expectancy, but did not predict outcome. It is likely that
in contexts where expectancy is more important, References
then optimism will correlate with outcome but be mediated
[1] Rajagopal S. The placebo effect. Psychiatri Bull 2006;30:185 – 8.
via expectancy. [2] Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H. The
The interpretation of our results should be treated with role of expectancies in the placebo effect and their use in the
caution. Although the motivational explanation works well delivery of health care: a systematic review. Health Technol Assess
for gratitude therapy, there remains a question mark over its 1999;3:1 – 96.
application to flower essence therapy. Our explanation [3] Shapiro AK. A historic and heuristic definition of the placebo.
Psychiatry 1964;27:52 – 8.
requires participants to interpret flower essences as a [4] Stewart-Williams S. The placebo puzzle: putting together the pieces.
spiritual therapy. Edward Bach, the inventor of flower Health Psychol 2004;23:198 – 206.
essences, suggested a spiritual interpretation of illness, but it [5] Kirsch I. Placebo psychotherapy: synonym or oxymoron? J Clin
is unlikely that many participants would have read Bach’s Psychol 2005;61:791 – 803.
[6] Wampold BE. The great psychotherapy debate: models, methods, and
philosophical writings. How and whether flower essences
findings. Hillside (NJ)7 Erlbaum, 2001.
came to be interpreted as spiritual by ordinary people [7] Stewart-Williams S, Podd J. The placebo effect: dissolving the
remains unclear. Nevertheless, we have replicated the expectancy versus conditioning debate. Psychol Bull 2004;130:
correlation between spirituality and flower essence outcome, 324 – 40.
showing that this correlation is unlikely to be an artifact. We [8] Kirsch I. Conditioning, expectancy, and the placebo effect: com-
cannot rule out other, as yet unknown, explanations for the ment on Stewart-Williams and Podd (2004). Psychol Bull
2004;130:341 – 3.
relationship between spirituality and outcome in flower [9] Montgomery GH, Kirsch I. Classical conditioning and the placebo
essences. Whether or not our explanation for flower effect. Pain 1997;72:107 – 13.
essences is correct, we feel confident, on the basis of the [10] Brody H. The placebo response. New York7 HarperCollins, 2000.
gratitude therapy finding, that there is a motivational [11] Moerman D. Meaning, medicine, and the bplacebo effectQ.
Cambridge7 Cambridge Univ Press, 2002.
mechanism underlying therapeutic rituals. Whether such
[12] Fisher S, Greenberg RP. The curse of the placebo: fanciful pursuit of a
therapeutic rituals should be labeled placebo or positive pure biological therapy. In: Fisher S, Greenberg RP, editors.
psychology is a matter of terminology that extends beyond From placebo to panacea: putting psychiatric drugs to the test. Wiley,
the scope of this paper. Certainly one can argue that the 1997. pp. 3 – 56.
word placebo fails to do justice to the several psychological [13] Geers AL, Handley IM, McLarney AR. Discerning the role of
processes underlying therapeutic rituals. optimism in persuasion: the valence-enhancement hypothesis. J Pers
Soc Psychol 2003;85:554 – 65.
[14] Ernst E, White A. The BBC survey of complementary medicine use in
the UK. Complement Ther Med 2000;8:32 – 6.
Conclusion [15] Thomas KJ, Nicholl JP, Coleman P. Use and expenditure on
complementary medicine in England: a population based survey.
We believe we have resolved the controversy over the Complement Ther Med 2001;9:2 – 11.
existence of the dispositional placebo responder: Both those [16] Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary
and alternative medicine use among adults: United States, 2002.
who believe and those who do not believe in the idea of a
Semin Integr Med 2004;2:54 – 71.
placebo responder are correct. Our data suggest that there is [17] Shang A, Huwiler-Mqntener K, Nartey L, Jqni P, Dfrig S, Sterne
a Person  Situation interaction, and the context determines JAC, et al. Are the clinical effects of homoeopathy placebo effects?
the personality correlate. Failure to take motivational Comparative study of placebo-controlled trials of homoeopathy and
context into account may have contributed to previous allopathy. Lancet 2005;366:726 – 32.
inconsistencies in data. On the basis of our and other data [18] Raoult D. Are the clinical effects of homoeopathy placebo effects?—
Authors’ reply. Lancet 2006;366:2085 – 6.
[58,59], we believe that there is now evidence for a non- [19] Walach H, Jonas W, Lewith G. Are the clinical effects of homoeo-
expectancy-mediated, motivational mechanism whereby the pathy placebo effects? Lancet 2006;366.
positive experience of engaging in the therapeutic ritual has [20] Lewith GT, Watkins AD, Hyland ME, Shaw S, Broomfield JA, Dolan
health promoting benefits. Therapeutic rituals are effective G, et al. Use of ultramolecular potencies of allergen to treat asthmatic
due to several psychological mechanisms. people allergic to house dust mite: double blind randomised controlled
clinical trial. BMJ (Clinical Research Ed) 2002;324:520.
[21] Lewith GT, Hyland ME, Shaw S. Do attitudes toward and beliefs
about complementary medicine affect treatment outcomes? Am J
Acknowledgments Public Health 2002;92:1604 – 6.
[22] Ernst E, White AR. Acupuncture for back pain: a meta-analysis of
randomized controlled trials. Arch Intern Med 1998;158:2235 – 41.
Samantha Bampton, Sarah Deacon, James Freemantle, [23] Ernst E, White AR, Wider B. Acupuncture for back pain:
Jasmin Wheeler, and Philippa Wheeler helped collect data meta-analysis of randomised controlled trials and an update with data](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-9-2048.jpg)
![340 M.E. Hyland et al. / Journal of Psychosomatic Research 62 (2007) 331–340
from the most recent studies. Schmerz (Berlin, Germany) 2002;16: optimism, situational expectations, and the placebo response.
129 – 39. J Psychosom Res 2005;58:121 – 7.
[24] van Tulder MW, Furlan AD, Gagnier JJ. Complementary and [44] Hatch RL, Burg MA, Naberhaus DS, Hellmich LK. The spiritual
alternative therapies for low back pain. Best Pract Res Clin Rheumatol involvement and beliefs scale Development and testing of a new
2005;19:639 – 54. instrument. J Fam Pract 1998;46:476 – 86.
[25] Thomas K, MacPherson H, Thorpe L, Brazier J, Fitter M, Campbell [45] Hunglemann J, Kenkel-Rossi E, Klassen L, Stollenwerk R. Spiritual
M, et al. Longer term clinical and economic benefits of offering well-being in older adults: harmonious interconnectedness. J Relig
acupuncture to patients with chronic low back pain. Health Technol Health 1985;24:147 – 53.
Assess 2005;9:1 – 109. [46] Hyland M, Wheeler P. Empirical development of a spiritual scale for
[26] Walach H, Rilling C, Engelke U. Efficacy of Bach-flower remedies in psychosomatic research: the spiritual connection questionnaire.
test anxiety: a double-blind, placebo-controlled, randomized trial with Unpublished manuscript, 2006.
partial crossover. J Anxiety Dis 2001;15:359 – 66. [47] Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from
[27] Armstrong NC, Ernst E. A randomized, double-blind, placebo- neuroticism (and trait anxiety, self-mastery, and self-esteem): a
controlled trial of a Bach flower remedy. Complement Ther Nurs reevaluation of the Life Orientation Test. J Pers Soc Psychol 1994;
Midwifery 2001;7:215 – 21. 67:1063 – 78.
[28] Hyland ME, Geraghty AWA, Joy OET, Turner SI. Spirituality predicts [48] Hyland ME, Lewith GT, Westoby C. Developing a measure of
outcome independently of expectancy following flower essence self- attitudes: the holistic complementary and alternative medicine
treatment. J Psychosom Res 2006;60:53 – 8. questionnaire. Complement Ther Med 2003;11:33 – 8.
[29] Jensen MP, Karoly P. Motivation and expectancy factors in symptom [49] Oberbaum M, Singer SR, Vithoulkas G. The colour of the
perception: a laboratory study of the placebo effect. Psychosom Med homeopathic improvement: the multidimensional nature of the
1991;53:144 – 52. response to homeopathic therapy. Homeopathy 2005;94:196 – 9.
[30] Horwitz RI, Horwitz SM. Adherence to treatment and health [50] Schumann A, Hapke U, Meyer C, Rumpf H-J, John U. Measuring
outcomes. Arch Intern Med 1993;153:1863 – 8. sense of coherence with only three items: a useful tool for population
[31] Horwitz RI, Viscoli CM, Berkman L, Donaldson RM, Horwitz SM, surveys. Br J Health Psychol 2003;8:409 – 21.
Murray CJ, et al. Treatment adherence and risk of death after a [51] Gosling SD, Vazire S, Srivastava S, John OP. Should we trust Web-
myocardial infarction. Lancet 1990;336:542 – 5. based studies? A comparative analysis of six preconceptions about
[32] Carver CS, Scheier MF. On the self-regulation of behavior. New York7 Internet questionnaires. Am Psychol 2004;59:93 – 104.
Cambridge University Press, 1998. [52] Davis C, Ralevski E, Kennedy SH, Neitzert C. The role of personality
[33] Carver CS, Scheier MF. Control theory: a useful conceptual frame- factors in the reporting of side effect complaints to moclobemide and
work for personality—social, clinical, and health psychology. Psychol placebo: a study of healthy male and female volunteers. J Clin
Bull 1982;92:111 – 35. Psychopharmacol 1995;15:347 – 52.
[34] Hyland ME. Motivational control theory: an integrative framework. [53] Geers AL, Weiland PE, Kosbab K, Landry SJ, Helfer SG. Goal
J Pers Soc Psychol 1988;55:642 – 51. activation, expectations, and the placebo effect. J Pers Soc Psychol
[35] Sheldon KM, Elliot AJ. Goal Striving, need satisfaction, and 2005;89:143 – 59.
longitudinal well-being: the self-concordance model. J Pers Soc [54] Emmons RA, McCullough ME. Counting blessings versus burdens:
Psychol 1999;76:482 – 97. an experimental investigation of gratitude and subjective well-being in
[36] Gollwitzer P, Wicklund RA. The pursuit of self-defining goals. In: daily life. J Pers Soc Psychol 2003;84:377 – 89.
Kuhl R, Beckmann J, editors. Action control: from cognition to [55] McCullough ME, Emmons RA, Tsang J-A. The grateful disposition: a
behavior. Heidelberg (Germany)7 Springer-Verlag, 1985. conceptual and empirical topography. J Pers Soc Psychol 2002;
[37] Deci EL, Ryan RM. Intrinsic motivation and self-determination in 82:112 – 27.
human behavior. New York7 Plenum Press, 1985. [56] McCullough ME, Tsang J-A, Emmons RA. Gratitude in intermedi-
[38] Higgins ET. Self-discrepancy: a theory relating self and affect. ate affective terrain: links of grateful moods to individual differ-
Psychol Rev 1987;94:319 – 40. ences and daily emotional experience. J Pers Soc Psychol 2004;86:
[39] Frank J, Frank J. Persuasion and healing: a comparative study 295 – 309.
of psychotherapy. 3rd ed. Baltimore7 John Hopkins University Press, [57] Marino J, Gwynn MI, Spanos NP. Cognitive mediators in the
1991. reduction of pain: the role of expectancy, strategy use, and self-
[40] Maslow AJ. Motivation and personality. New York7 Harper & Row, presentation. J Abnorm Psychol 1989;98:256 – 62.
1970. [58] Devine DP, Spanos NP. Effectiveness of maximally different cognitive
[41] Bach E. Heal thyself; an explanation of the real cause and cure of strategies and expectancy in attenuation of reported pain. J Pers Soc
disease. Wappingers Falls7 Beekman Books Inc, 1996. Psychol 1990;58:672 – 8.
[42] Petry JJ, Finkel R. Spirituality and choice of health care practitioner. [59] Webb MS, Simmons VN, Brandon TH. Tailored interventions for
J Altern Complement Med 2004;10:939 – 45. motivating smoking cessation: using placebo tailoring to examine the
[43] Geers AL, Helfer SG, Kosbab K, Weiland PE, Landry SJ. influence of expectancies and personalization. Health Psychol
Reconsidering the role of personality in placebo effects: dispositional 2005;24:179 – 88.](https://image.slidesharecdn.com/hyland2007dispositionalpredictorsofplaceboresponding-120612104808-phpapp02/75/Hyland2007-dispositional-predictors-of-placebo-responding-10-2048.jpg)


















































![Coded Agents – with UiPath SDK + LangGraph [Virtual Hands-on Workshop]](https://cdn.slidesharecdn.com/ss_thumbnails/codedagentsdeck-251215155422-5497c599-thumbnail.jpg?width=640&height=640&fit=bounds)













