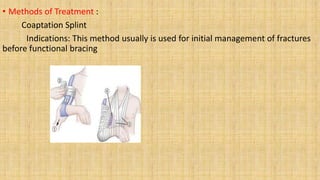
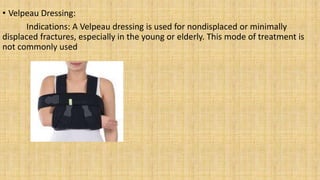
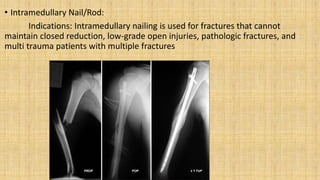
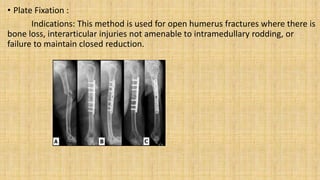
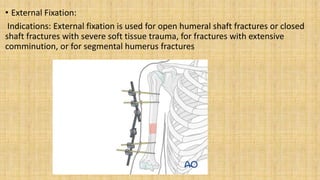
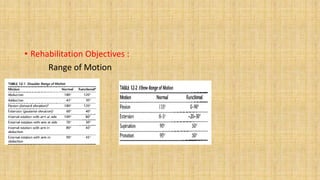
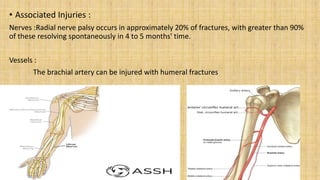
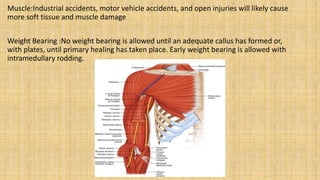
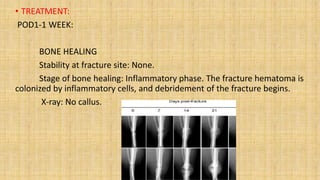
The document outlines the management of humeral shaft fractures, detailing mechanisms of injury, treatment methods, and rehabilitation protocols. Various treatment options include coaptation splints, Velpeau dressings, intramedullary nails, plate fixation, and external fixation, each with specific indications based on fracture type. It emphasizes rehabilitation objectives, expected healing durations, and the importance of assessing associated injuries and functional recovery throughout the healing process.