Download to read offline
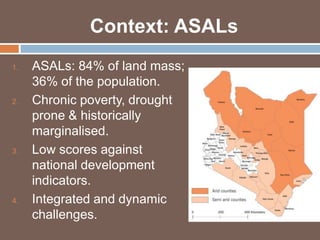



The Hunger Safety Net Programme (HSNP) is an unconditional cash transfer initiative aimed at reducing poverty and food insecurity in Kenya's arid and semi-arid lands by providing financial support to vulnerable households. Implemented in phases, the program has demonstrated effectiveness in improving food security, asset retention, and overall well-being, particularly in times of crisis, such as droughts. The second phase aims to expand the program's reach and sustainability, with an emphasis on improving targeting methods and maintaining strong oversight of fund distribution and beneficiary engagement.













































































