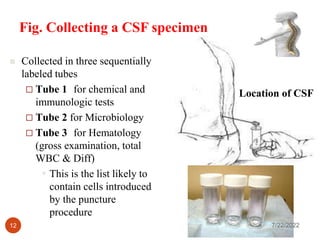
This document discusses cell counts on cerebrospinal fluid (CSF) and other body fluids. It defines CSF and other serous fluids like pleural, pericardial, and synovial fluid. The analysis and clinical significance of CSF is explained, including how to perform cell counts, quality control measures, and sources of error. A normal CSF analysis includes a gross examination, cell count and differential count, and measurements of glucose and protein. An increased number of neutrophils in the CSF differential count indicates bacterial infection or meningitis.

































































![CSF CNS covered by 3 membranes [meninges] pdf](https://cdn.slidesharecdn.com/ss_thumbnails/csf-240227110022-60ed50a9-thumbnail.jpg?width=640&height=640&fit=bounds)












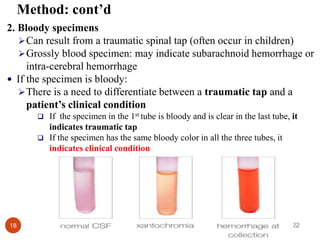
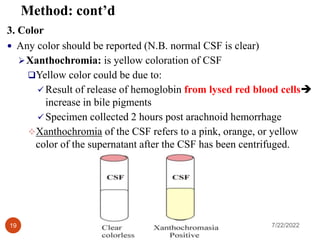
![Wude.dox[1].docx](https://cdn.slidesharecdn.com/ss_thumbnails/wude-220722173028-160755b3-thumbnail.jpg?width=640&height=640&fit=bounds)
![ADBMS_ASSIGNMENT_PPT1[1] (2).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/adbmsassignmentppt112-220722180655-7efe2464-thumbnail.jpg?width=640&height=640&fit=bounds)





















