Downloaded 18 times
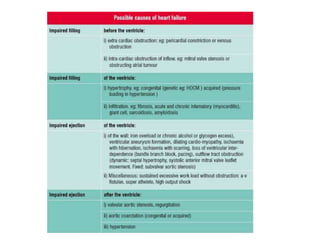
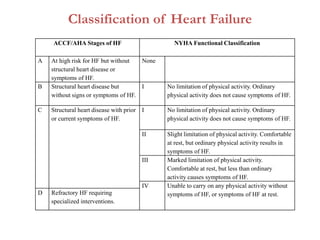
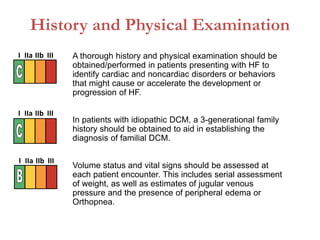

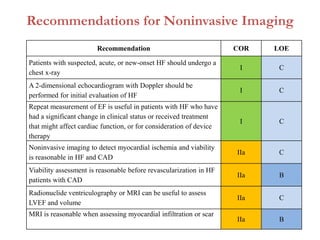
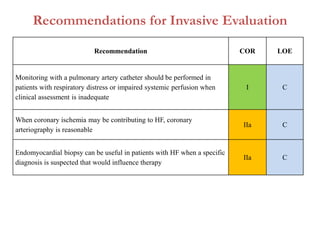
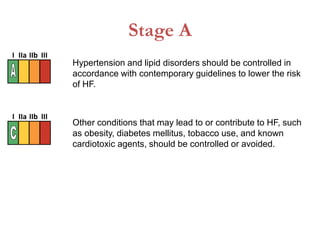
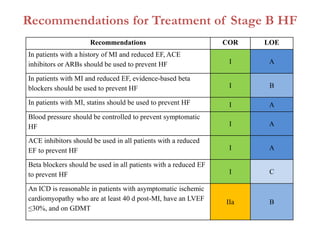
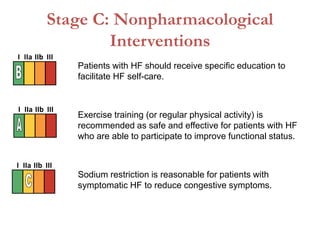
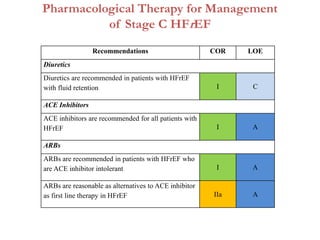
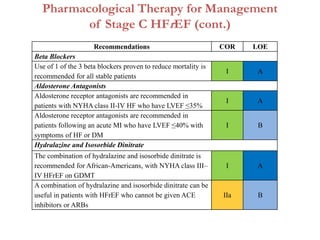
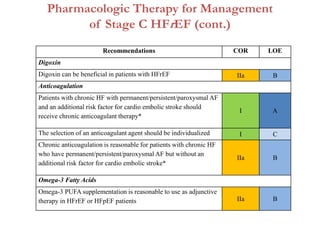
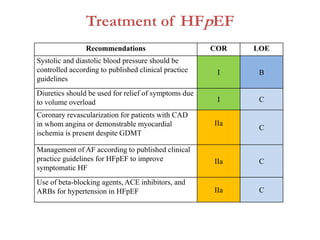
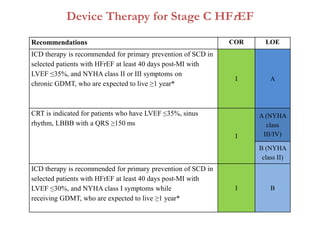
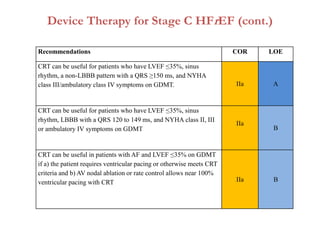
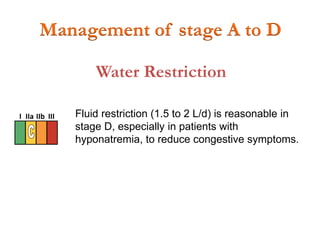
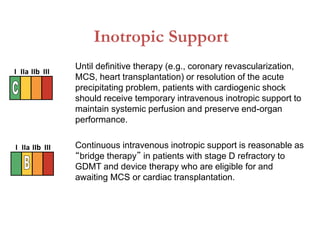
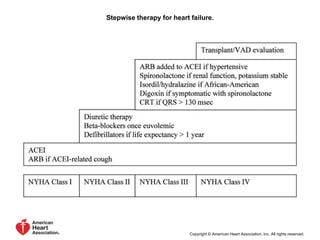

This document provides an overview of heart failure, including: 1. It defines heart failure and classifies it based on ACCF/AHA stages and NYHA functional classification. 2. It outlines recommendations for diagnostic tests, noninvasive imaging, invasive evaluation, and pharmacological and nonpharmacological treatment for stages A through D. 3. It discusses surgical interventions for heart failure such as ventricular reduction procedures, coronary artery bypass grafting, valve surgery, and cardiac transplantation.







































![slide-set-heart-failure-management [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/slide-set-heart-failure-managementautosaved-231110194029-14a57f1e-thumbnail.jpg?width=640&height=640&fit=bounds)



























