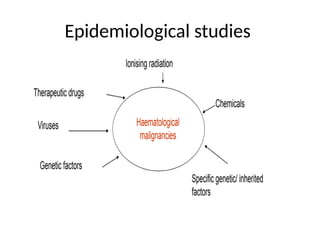
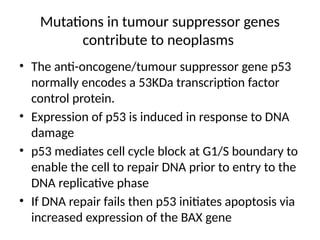
The document examines the aetiology and epidemiology of haematological malignancies, highlighting various causative factors including ionising radiation, chemicals, viruses, and genetic alterations. It discusses the impact of environmental exposures, therapeutic agents, and inherited genetic conditions on the development of these malignancies. Additionally, it details the molecular mechanisms behind malignancy, such as chromosomal translocations, point mutations, and the role of oncogenes and tumor suppressor genes.

![Inversions
• Inversions – AML inv(16)(p13.1q32) or t(16:16)
(p13.1q32), [M2 in FAB classification] results in
chimeric transcription factor which inhibits
normal maturation and development of
haematopoietic cells
– inv(3) (q21q26) are noted in a small proportion of
AML patients of M1, M2, M4, M6 and M7 sub-types.
• This inversion confers tri-lineage myelodysplasia
with notable abnormalities in the
megakaryocytic series](https://image.slidesharecdn.com/haematologicalmaligaethiology-241021130020-b5171b62/85/haematological-malignancy-aethiology-pptx-28-320.jpg)

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



