Introduction
• Gout isan inflammatory arthritis caused by hyperuricemia.
• It results from urate crystal deposition in joints and soft
tissues, triggering inflammation.
• Commonly affects the first metatarsophalangeal (MTP) joint
(podagra) but can involve other joints.
• Can progress to chronic gouty arthritis if untreated.
3.
Epidemiology
• More prevalentin men (especially >40 years) and
postmenopausal women.
• Increasing global prevalence due to aging populations and
dietary changes.
• Higher incidence in developed countries due to increased
consumption of purine-rich foods and alcohol.
4.
Risk Factors forGout
Non-Modifiable:
• Age (>40 years) and male sex.
• Genetic predisposition (e.g., reduced uric acid excretion).
Modifiable:
• High-purine diet (red meat, seafood, alcohol).
• Obesity and metabolic syndrome.
• Medications (diuretics, cyclosporine, low-dose aspirin).
5.
Pathophysiology
• Gout isan inflammatory form of arthritis caused by the deposition of
monosodium urate (MSU) crystals in joints and tissues due to
hyperuricemia, which is elevated levels of uric acid in the blood.
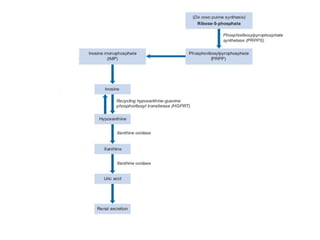
• Uric acid is produced as the end product of purine metabolism, where
purines are broken down into hypoxanthine, xanthine, and finally uric
acid by the enzyme xanthine oxidase.
• Uric acid is typically excreted by the kidneys, with a small amount
excreted through the gastrointestinal tract.
• However, in gout, there is either excessive production of uric acid,
often from high-purine foods, alcohol consumption, or increased cell
turnover, or insufficient renal excretion, particularly in conditions like
chronic kidney disease or the use of diuretics.
7.
• When serumuric acid levels exceed its solubility limit
(usually 6.8 mg/dL), uric acid crystals precipitate and
accumulate in joints, with the cooler areas of the body like the
big toe being most commonly affected.
• These crystals trigger an immune response, activating
neutrophils and macrophages, which release inflammatory
mediators such as interleukins, prostaglandins, and
leukotrienes, causing intense pain, swelling, and redness—
hallmarks of a gout flare.
• Over time, persistent hyperuricemia can lead to the formation
of tophi, large deposits of urate crystals that can damage joints
and surrounding tissues.
• Chronic hyperuricemia also increases the risk of uric acid
kidney stones and nephropathy.
8.
Clinical Features
Acute Gout:
•Sudden onset of severe pain, redness, and swelling in a single
joint.
• Commonly affects the big toe (podagra), but can involve
knees, ankles, etc.
Chronic Gout:
• Recurrent flares lead to chronic arthritis.
• Tophi (urate deposits) develop in joints and soft tissues.
• Associated with kidney stones due to uric acid precipitation.
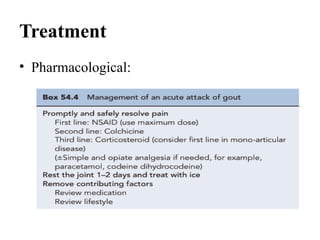
NSAIDs
Diclofenac
• Dose: 50mg 2-3 times/day (oral).
• MOA: Inhibits COX-1 and COX-2 enzymes, reducing prostaglandin
synthesis.
• ADR: GI upset, renal issues, cardiovascular risk, liver toxicity (rare).
Ibuprofen
• Dose: 400-800 mg every 6-8 hours (oral).
• MOA: Inhibits COX-1 and COX-2 enzymes to reduce inflammation.
• ADR: GI upset, renal issues, cardiovascular risk, hypersensitivity (rash,
bronchospasm).
Naproxen
• Dose: 500 mg initially, then 250 mg every 8 hours (oral).
• MOA: Inhibits COX-1 and COX-2 to decrease inflammation.
• ADR: GI bleeding, renal impairment, cardiovascular risk.
13.
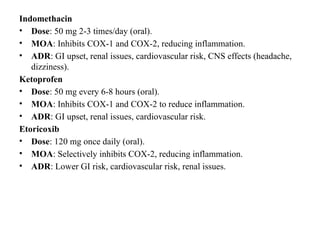
Indomethacin
• Dose: 50mg 2-3 times/day (oral).
• MOA: Inhibits COX-1 and COX-2, reducing inflammation.
• ADR: GI upset, renal issues, cardiovascular risk, CNS effects (headache,
dizziness).
Ketoprofen
• Dose: 50 mg every 6-8 hours (oral).
• MOA: Inhibits COX-1 and COX-2 to reduce inflammation.
• ADR: GI upset, renal issues, cardiovascular risk.
Etoricoxib
• Dose: 120 mg once daily (oral).
• MOA: Selectively inhibits COX-2, reducing inflammation.
• ADR: Lower GI risk, cardiovascular risk, renal issues.
14.
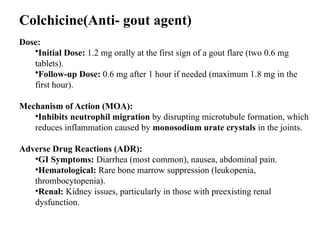
Colchicine(Anti- gout agent)
Dose:
•InitialDose: 1.2 mg orally at the first sign of a gout flare (two 0.6 mg
tablets).
•Follow-up Dose: 0.6 mg after 1 hour if needed (maximum 1.8 mg in the
first hour).
Mechanism of Action (MOA):
•Inhibits neutrophil migration by disrupting microtubule formation, which
reduces inflammation caused by monosodium urate crystals in the joints.
Adverse Drug Reactions (ADR):
•GI Symptoms: Diarrhea (most common), nausea, abdominal pain.
•Hematological: Rare bone marrow suppression (leukopenia,
thrombocytopenia).
•Renal: Kidney issues, particularly in those with preexisting renal
dysfunction.
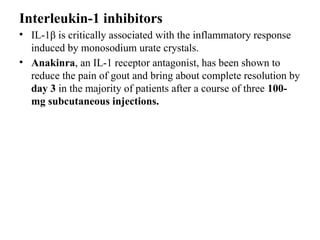
Interleukin-1 inhibitors
• IL-1βis critically associated with the inflammatory response
induced by monosodium urate crystals.
• Anakinra, an IL-1 receptor antagonist, has been shown to
reduce the pain of gout and bring about complete resolution by
day 3 in the majority of patients after a course of three 100-
mg subcutaneous injections.
17.
Chronic Gout
• Uricostaticagents act on the enzyme xanthine oxidase.
Xanthine oxidase catalyses the oxidation of hypoxanthine to
xanthine and subsequently xanthine to uric acid.
• Uricosuric agents increase uric acid excretion primarily by
inhibiting post-secretory tubular absorption of uric acid from
filtered urate in the kidney.
• Uricolytic drugs convert uric acid to allantoin through the
actions of the enzyme urate oxidase (uricase). Uricolytics are
indicated for hyperuricaemia associated with tumour lysis
syndrome and are not indicated for other forms of
hyperuricaemia.
21.
Allopurinol
• Dose: 100mg/day; this is gradually increased in 100-mg incre ments every 2–3
weeks until the optimal serum urate level
• MOA: Xanthine oxidase inhibitor; reduces uric acid production by inhibiting
xanthine oxidase.
• ADR: Rash, GI upset, liver enzyme elevation, hypersensitivity, bone marrow
suppression.
Febuxostat
• Dose: 40-80 mg/day
• MOA: Selective xanthine oxidase inhibitor; decreases uric acid production
more specifically than allopurinol.
• ADR: Hepatotoxicity, rash, nausea, cardiovascular events (heart attacks,
stroke), elevated liver enzymes.
Sulfinpyrazone
• Dose: 50-400 mg/day (titrated)
• MOA: Uricosuric agent; increases renal excretion of uric acid by inhibiting its
reabsorption.
• ADR: GI upset, rash, kidney stones, hematologic effects (e.g.,
thrombocytopenia).
22.
Probenecid
• Dose: 250-1000mg/day
• MOA: Uricosuric agent; inhibits renal reabsorption of uric
acid, increasing its excretion.
• ADR: GI upset, rash, kidney stones, headache.
Benzbromarone
• Dose: 100-200 mg/day
• MOA: Uricosuric agent; enhances uric acid excretion by
inhibiting reabsorption in the kidneys.
• ADR: GI upset, rash, headache, kidney stones.
23.
Pegloticase
• Dose: 8mg IV every 2 weeks
• MOA: Converts uric acid to allantoin (highly soluble) via recombinant
uricase
• ADRs:
– Severe infusion reactions, anaphylaxis
– Hemolysis
– Anti-drug antibodies (reduces efficacy)
Rasburicase
• Dose: 0.2 mg/kg IV once daily for up to 5 days
• MOA: Converts uric acid to allantoin via recombinant uricase
• ADRs:
– Hypersensitivity, anaphylaxis
– Hemolysis
– Fever, nausea
24.
Non-Pharmacological Management
• Diet:Reduce purine-rich foods (red meat, seafood, alcohol).
• Hydration: >2L/day to prevent kidney stones.
• Weight loss: Reduces uric acid production and improves renal
clearance.
• Alcohol restriction: Especially beer and spirits (high purine
content).
























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







