Glaucoma
•
14 likes•1,299 views

one of my education lecture in ophthalmic hospital about glaucoma patho-physiology and management as illustrated in applied therapeutic 10th edition - clinical pharmacy department

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Glaucoma
Similar to Glaucoma (20)
More from Hemat Elgohary
More from Hemat Elgohary (9)
Recently uploaded
Recently uploaded (20)
Glaucoma
- 1. Glaucoma clinical pharmacy department :Dr.Hemat Elgohary1-12-2016
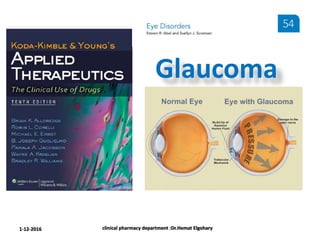
- 2. Increased intraocular pressure (IOP) is the most common risk factor for the development of glaucoma Even people with “normal” IOPS can experience vision loss from glaucoma. the higher the IOP is, the greater the risk for developing glaucoma. Glaucoma Leading cause of blindness worldwide A nonspecific term used for a group of diseases that can irreversibly damage the optic nerve resulting in visual field loss. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 3. Other risk factors for glaucoma. Increasing age African american race Family history Thinner central corneas Larger vertical cup-disc ratios clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 4. Intraocular Pressure The inner pressure of the eye (IOP) is influenced by : The production of aqueous humor by the ciliary processes The outflow of aqueous humor through the trabecular meshwork. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 5. although a more rare form of glaucoma is associated with a low IOP. The Tonometry test to measure the IOP is based on the pressure required to flatten a small area of the central cornea. IOP of 10 to 20 mm Hg is considered normal. IOP of 22 mm Hg or greater should arouse suspicion of glaucoma 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary
- 6. Ocular Hypertension Ocular hypertension has been defined as : 1) An IOP exceeding 21 mm hg 2) Normal visual fields 3) Normal optic discs 4) Open angles 5) The absence of any ocular disease contributing to the elevation of IOP. Only a small percentage of patients with ocular hypertension have open-angle glaucoma. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary
- 7. An ophthalmoscope Can examine the inside of the eye Especially the optic nerve Diagnosis of glaucoma can be applied when pathologic cupping of the optic nerve is observed. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 8. Open-Angle Glaucoma Primary open-angle glaucoma occurs in about 1.8% of people older than 40 years of age glaucoma can affect other age groups, including children. About 2.2 million people have glaucoma this number likely will increase to about 3.3 million by the year 2020 as the population ages. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 9. aqueous humor outflow from the anterior chamber is continuously subnormal primarily because of a degenerative process in the trabecular meshwork. In patients with primary open-angle glaucoma (POAG) The IOP can vary in the course of a day from normal to significantly high pressures clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 10. The decreased outflow appears to : be caused by degenerative changes in outflow channels (i.e., the trabecular meshwork and Schlemm canal) and tends to worsen with the passage of time. In rare cases, the outflow is normal even during a phase of elevated IOP, and the elevation appears to be to the result of hyper-secretion of aqueous humor. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 11. Visual field defects A defect in the visual field examination may be present in early glaucoma but loss of peripheral vision usually is not seen until late in the course of the disease. Visual field defects correlate well with changes in the optic disc and help differentiate glaucoma from ocular hypertension in patients with increased IOP. The onset of POAG usually is gradual and asymptomatic. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 12. Patients with : normal visual fields IOP of 24 mm Hg or greater have a 10% likelihood of developing glaucoma in 5 years. Examination of the anterior chamber angle by : Gonioscopy using a corneal contact lens a magnifying device (e.g., a slit-lamp microscope) a light source assists in differentiating between open-angle glaucoma and angle-closure glaucoma. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 13. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 14. Angle-closure glaucoma accounts for approximately 5% to 10% of all primary glaucoma cases. The sole cause of the elevated IOP in angle-closure glaucoma is closure of the anterior chamber angle. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 15. When patients are predisposed to angle-closure glaucoma Their pupils should not be dilated (e.g., During an ophthalmic examination) And they should be taught the signs and symptoms of angle closure. Angle-closure glaucoma, which is : 1. A medical emergency 2. Usually presents as an acute attack 3. With a rapid increase in IOP 4. Blurring or sudden loss of vision 5. Appearance of haloes around lights 6. Pain that is often severe clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 16. Permanent medical management of acute or chronic angle-closure glaucoma is difficult: surgical procedures (e.g., peripheral irid-ectomies) often are needed Acute attacks can terminate without treatment But if the IOP remains high, the optic nerve can be irreparably damaged. Patients with chronic angle-closure generally experience a gradual closure of aqueous humor outflow channels, and patients can be asymptomatic until the glaucoma is in an advanced stage. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 17. PRIMARY OPEN-ANGLE GLAUCOMA Therapeutic Agents for Treatment of Primary Open-Angle Glaucoma Historically, β-adrenergic blockers have been the most commonly prescribed first-line agents for the treatment of POAG. In recent years, prostaglandin analog use has reached, if not exceeded, β-adrenergic blocker use. All of the ophthalmic β- blockers currently on the market are available in generic formulation allowing for cost-effective treatment. generic versions of prostaglandin analogs are not yet available the cost be prohibitive for some patients, depending on their insurance plans clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 18. β -ADRENERGIC BLOCKERS clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 19. block the β-adrenergic receptors in the ciliary epithelium of the eye lower IOP primarily by decreasing aqueous humor production. β-blockers decrease IOP by 20% to 35% depending on : 1. The strength used 2. The frequency of administration. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 20. Timolol (Timoptic) Nonselective β1- and β2-adrenergic antagonist one of the most commonly prescribed glaucoma medications. Because Timolol was the first ocular β- adrenergic blocker marketed marketed ophthalmic β-blockers usually are compared with Timolol for safety and effectiveness. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 21. Monocular administration of Timolol has resulted in equal bilateral IOP reduction and can reduce the cost of therapy and side effects for some patients. Concentrations or dosages exceeding one drop of Timolol 0.5% twice daily (BID) DO NOT produce further significant decreases in IOP. Therapy usually is initiated with a 0.25% solution administered as one drop BID. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 22. An escape phenomenon or tachyphylaxis, can occur with timolol. Timolol has been associated with a modest reduction of resting pulse rate (5–8 beats/minute) worsening of heart failure adverse pulmonary effects (e.g., dyspnea, airway obstruction, pulmonary failure). S.E After chronic administration in susceptible individuals, timolol can cause corneal anesthesia. Although uveitis has been reported in patients receiving ophthalmic timolol, a cause-and-effect relationship has not been established. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 23. Systemic absorption after topical administration does occur, but it may not be significant in the majority of patients. Care should be taken when timolol is used in patients with: Sinus brady-cardia Heart failure Pulmonary disease. Systemic side effects could be exaggerated in Elderly patients secondary to : inadvertent overdosing associated with poor administration technique . clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 24. Timolol ophthalmic gel-forming solution, is administered once daily. The ophthalmic vehicle, gellan gum(gelrite), is a solution that forms a clear gel in the presence of monovalent or divalent cations. This ion-activated gelation : prolongs pre-corneal residence time increases ocular bioavailability allowing timolol to be administered once daily. Timoptic xe is comparable to timoptic solution in lowering IOP. Timoptic XE clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 25. Levobunolol 0.5% and 1% are comparable to timolol in lowering IOP. The incidence of adverse reactions, including decreases in heart rate, are also comparable to that for timolol. Levo-buno-lol (Betagan) Nonselective β-adrenergic antagonist approved for either once daily or BID administration clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 26. Metipranolol is associated with: a greater incidence of stinging or burning on administration granulomatous anterior uveitis. Meti-prano-lol (OptiPranolol) Nonselective β-adrenergic blocking agent Metipranolol 0.1% to 0.6%, is comparable to timolol 0.25% to 0.5% in reducing IOP. Like timolol, metipranolol produces corneal anesthesia,which occurs within 1 minute of instillation and returns to baseline after 10 minutes. As a result of these side effects, the use of metipranolol is limited. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 27. Carteolol 1% and Timolol 0.25% administered BID are equally effective in reducing IOP. Carteo-lol (Ocupress) nonselective β-adrenergic blocking agent with partial β-adrenergic agonist activity Theoretically should minimize the bronchospastic, bradycardic, and hypotensive effects associated with other ocular β-adrenergic blockers. no clinical differences were seen when the cardiovascular and pulmonary function effects of carteolol were compared with those of timolol. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 28. Betaxolol is slightly less effective than timolol in IOP reduction more patients tend to need adjunctive therapy with betaxolol. Beta-xo-lol (Betoptic) selective β1-adrenergic blocker. This cardio-selective property may result in less adverse effects on pulmonary function than nonselective β-adrenergic blockers in patients with reactive airway disorders. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 29. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary Timolol, and possibly all other Ḃ-blockers, have minimal IOP-lowering efficacy during sleep.
- 30. Prostaglandin analogs clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 31. Latanoprost (Xalatan) travoprost (Travatan) bimatoprost (Lumigan) clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 32. These agents often are prescribed as first-line agents for the treatment of POAG because they are : 1) At least as effective as the β-blockers 2) Can be administered once a day 3) Are associated with minimal systemic adverse effects. Latanoprost and travoprost are analogs of prostaglandin F2α , and they lower IOP by serving as selective prostaglandin F2α - receptor agonists. Bimatoprost is a synthetic prostamide analog. The prostaglandin analogs(PGAs) increase uveo- scleral outflow of aqueous humor and, thereby, decrease IOP. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 33. the nocturnal control of IOP with latanoprost was superior to that with timolol. Latanoprost Latanoprost 0.005% should be: dosed once daily in the evening because the IOP-lowering effects of latanoprost might actually be inferior when administered more frequently. Approved for the initial treatment of POAG or ocular hypertension. When administered once daily in the evening, latanoprost is at least as effective as timolol in decreasing iop. When the effectiveness of latanoprost 0.005% once daily was compared with timolol 0.5% BID, the IOP-lowering effects of latanoprost were superior to those of timolol. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 34. Systemic side effects are minimal with latanoprost local reactions are relatively common. 1. iris pigmentation 2. eyelid skin darkening 3. eyelash lengthening ,thickening, pigmentation, and misdirected growth 4. conjunctival hyperemia 5. ocular irritation 6. superficial punctate keratitis Latanoprost can gradually increase the amount of brown pigment in the iris by increasing the melanin content in the stromal melanocytes of the iris. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 35. The nature and severity of adverse events are not affected by the increased pigmentation of the iris. This pigment change occurs in 7% to 22% of patients and is most noticeable in those with green- brown, blue/gray brown,or yellow-brown eyes. The onset of increased iris pigmentation usually is noticeable within the first year of treatment and can be permanent. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 36. Latanoprost has additive effects when administered with : β-blockers (e.g., timolol) carbonic-anhydrase inhibitors (e.g.,dorzolamide) α2-adrenergic agonists (e.g., brimonidine,apraclonidine). When added to existing therapy, latanoprost decreases IOP an additional 2.9 to 6.1 mm Hg. As a result,latanoprost is a good adjunctive ophthalmic agent for patients who are unable to adequately lower their IOP with single-agent therapy. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 37. The complementary IOP-lowering effects of latanoprost are comparable with those of brimonidine (at least a 15% reduction in IOP) brimonidine (an α2-adrenergic agonist) in a comparative study was associated with fewer adverse effects on the quality of life. in patients inadequately controlled on β-adrenergic blocking agents watery or teary eyes and cold hands and feet were reported more frequently in latanoprost treated patients. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 38. Travoprost Travoprost (Travatan Z) is US Food and Drug Administration (FDA)–approved for the reduction of elevated IOP and ocular hypertension in patients who are intolerant or who fail to respond to other agents. Travoprost is used as a first-line agent in clinical practice because it is more effective than timolol and at least as effective as latanoprost. The mean IOP reduction with travoprost in African American patients was 1.8 mm Hg greater than in non–African American patients. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 39. Travoprost, as adjunctive therapy to timolol in patients not responding adequately to timolol alone, reduced IOP an additional 6 to 7 mm Hg. The side-effect profile of travoprost is similar to that for latanoprost, including increased iris pigmentation and eyelash changes. Local irritation may be less because it is free of the preservative benzalkonium chloride. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 40. Bimatoprost once daily or BID achieved lower target IOPs than did timolol BID. Bimatoprost BID, however, was less effective than bimatoprost once a day. Iris pigmentation changed in 1.1% of bimatoprost treated patients. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 41. Side effects were similar between treatment groups conjunctiva hyperemia was more common ( p <0.001) in bimatoprost treated patients. Overall, the side effect profile of bimatoprost appears to be similar to that for latanoprost and travoprost. The local side effects seen with other PGAs also appear to be relatively common with bimatoprost. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 42. Eyelash lengthening Thickening darkening or pigmentation is seen after 8 to 16 weeks of use. the FDA approved the cosmetic use of bimatoprost solution Latisse Latisse solution is applied with an applicator to the base of the upper eyelashes for the treatment of hypotrichosis (inadequate eyelashes). clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 43. α2-Adrenergic Agonists clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 44. Apraclonidine (Iopidine) brimonidine (Alphagan) Are selective α2-adrenergic agonists similar to clonidine. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 45. Less lipophilic than clonidine and brimonidine Does not cross the blood–brain barrier as readily Apraclonidine Theoretically has fewer systemic side effects 1. Hypotension 2. Decreased pulse 3. Dry mouth Apraclonidine 1% indicated to control or prevent post-surgical elevations in IOP after Argon laser trabeculoplasty or iridotomy. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 46. Common ocular side effects include 1. Burning 2. Stinging 3. Blurring 4. conjunctival follicles 5. An Allergic like reaction consisting of hyperemia, pruritus, edema of the lid and conjunctiva, and foreign body sensation. The 0.5% apraclonidine solution is indicated for short-term adjunctive therapy in patients on maximally tolerated medical therapy. Long-term IOP control should be monitored closely in patients taking α2- adrenergic agonists because tachyphylaxis can occur. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 47. It may also be used as adjunctive therapy in patients not responding to other agents. Brimonidine more highly selective for α2-adrenergic receptors than clonidine or apraclonidine Theoretically, should be associated with fewer ocular side effects. α2-Adrenergic agonists appear to lower IOP by decreasing the production of aqueous humor and by increasing uveo-scleral outflow. Brimonidine is an alternative first-line agent in the treatment of POAG. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 48. α2-Adrenergic agonists should be used with caution in patients with : 1. cardiovascular disease 2. orthostatic hypotension 3. Depression 4. renal or hepatic dysfunction Although ocular side effects are less common with brimonidine than with apraclonidine, systemic side effects are more common with brimonidine e.g. 1. dry nose and mouth 2. mild hypotension 3. decreased pulse 4. Lethargy clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 49. Brimonidine (Alphagan P) Is available with purite as a preservative, which: facilitates drug delivery into the eye allowing use of a lower drug concentration. The IOP-reduction effects (peak and trough) of brimonidine 0.2% BID are 14% to 28%. Although the approved dosing schedule of brimonidine is Three Times A Day (TID), brimonidine 0.2% BID lowers IOP comparably to timolol 0.5% BID,and both are slightly better than betaxolol 0.25% BID. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 50. The IOP-lowering effect of brimonidine also may be comparable with that of latanoprost; however, conflicting efficacy and tolerability results in clinical studies may be related to differences in study design. is as equally tolerable and effective as the combination brimonidine and timolol dorzolamide and timolol. The combination of clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 51. The FDA-approved combines α2-adrenergic agonist (brimonidine tartrate 0.2%) β-adrenergic blocker (timolol maleate 0.5%). Combigan ophthalmic clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 52. Topical carbonic anhydrase inhibitors clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 53. Although CAIs have been used orally for many years in the treatment of elevated IOPs, they have been replaced by the topical ophthalmic CAIs Carbonic anhydrase occurs in high concentrations in the ciliary processes and retina of the eye. resulting in a 40% to 60% decrease in aqueous humor secretion. Bicarbonate production Carbonic anhydrase inhibitors (CAIs) lower IOP by Bicarbonate Sodium water the posterior chamber clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 54. Dorzol-amide (Trusopt) Brinzol-amide (Azopt) which are safer and better tolerated. Topical CAIs are excellent alternatives to β-blockers in the initial management of elevated IOPs, and are effective as adjunctive agents. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 55. Brinzolamide 1% TID reduces IOP comparably to that achieved with dorzolamide 2% TID and to betaxolol 0.5% BID, but slightly less than timolol 0.5% BID. The IOP-reduction effects (peak and trough) of dorzolamide 2% TID are 16% to 25%. Brinzolamide and dorzolamide are approved for TID dosing; however, BID dosing may be adequate. Dorzolamide provides additional IOP-lowering effects when added to existing β-blocker therapy. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 56. The combined use of topical dorzolamide and oral acetazolamide does not result in additive effects and might increase the risk of toxicity. An ophthalmic solution of dorzolamide hydrochloride and timolol maleate is marketed as Cosopt. The topical CAIs are well tolerated with few systemic side effects. The most common adverse effects with dorzolamide are : 1. ocular burning 2. Stinging 3. discomfort and allergic reactions 4. bitter taste 5. superficial punctate keratitis.clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 57. These drugs should not be used in patients with renal or hepatic impairment. Brinzolamide dorzolamide causes less burning and stinging of the eyes, because its pH more closely resembles that of human tears. Both are sulfonamides and may cause the same types of adverse reactions attributable to sulfonamides. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 58. PILOCARPINE (Isopto Carpine) historically was an initial treatment of choice, but with the introduction and widespread use of newer agents, pilocarpine has fallen out of favor. M.O.A direct-acting cholinergic (parasympatho-mimetic) causes contraction of ciliary muscle fibers attached to the trabecular meshwork and scleralspur make it open to enhance aqueous humor outflow. There also may be a direct effect on the trabecular meshwork. Pilocarpine causes miosis by contraction of the iris sphincter muscle, but the miosis is not related to the decrease in IOP. Therapy usually is begun using lower concentrations (1%), one drop four times a day (QID).clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 59. CARBACHOL reserved as a third-line agent in patients who are unresponsive or intolerant to initial medications. In addition to having direct cholinergic effects, carbachol is more resistant to cholinesterase than pilocarpine. Added benefits include: increased release of acetylcholine from parasympathetic nerve terminals weak anticholinesterase effect. Carbachol is administered TID. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 60. Anticholinesterase agents If control of IOP is not achieved with : optimal use of other topical monotherapy combination therapy agents anticholinesterase agents may be prescribed as a last topical therapy option. Acetylcholine cholinesterase Destruction Anticholinesterase clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 61. Echo-thio-phate iodide Echothiophate iodide (Phospholine Iodide), an irreversible cholinesterase inhibitor primarily inactivates pseudo cholinesterase and secondarily inhibits true cholinesterase. may be used if maximal doses of other agents and combination therapy are ineffective. has a long duration of action that affords good control of IOP miosis and myopia are significant side effects. Concentrations higher than 0.06% are associated with a significant increase in subjective complaints (e.g., brow ache). clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 62. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary
- 63. Combination Therapy clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 64. In general, drugs with different pharmacologic actions have at least partially additive effects in lowering IOP in the treatment of glaucoma. Drugs with similar pharmacologic actions (i.e., from the same pharmacologic class) should not be combined because dose-related adverse effects are more likely and the incremental increase in benefits is likely to be more modest. Timolol and other β-adrenergic blocking drugs have additive IOP lowering effects when used in combination with : 1. miotic agents 2. prostaglandin analogs 3. α2-agonists 4. CAIs. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 65. For example, the IOP-lowering effect is greater when Timolol is used in combination with: 1. pilocarpine 2. Dorzolamide 3. Brimonidine 4. travoprost. Latanoprost has additive effects when administered with: 1. timolol 2. Dorzolamide 3. α2-adrenergic agonists clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 66. These advantages include : improved adherence because of a reduction in the number of dosages and bottles eliminating the need to instill two separate drugs 5 to 10 minutes apart to prevent a washout effect from the second medication improving safety and tolerability by limiting the exposure to the benzalkonium chloride preservative a cost savings for the patient by potentially eliminating a copay for one of the medications. The trend toward the development of fixed-combination products offers many advantages in the treatment of POAG. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 67. These investigational agents include Timolol/latanoprost (xalacom) Timolol/travoprost (duotrav, extravan) Timolol/bimatoprost. There are two β-adrenergic blocker combination products currently on the market timolol/dorzolamide (Cosopt) brimonidine/timolol (Combigan). The IOP-lowering effects of timolol/dorzolamide (Cosopt) are comparable to or greater than those of latanoprost monotherapy. Several other combination products are under investigation for POAG, which will offer a wide range of options for patients. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 68. Predisposing Factors clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 69. CASE 1 QUESTION 1: Tonometry measured an IOP of 36 mm Hg in both eyes. Ophthalmoscopy revealed physiologic cupping of the optic discs in both eyes visual field examination revealed a nerve fiber bundle defect consistent with glaucoma. Pupils were normal in both eyes, Gonioscopy indicated that anterior chamber angles were open in both eyes. There were no signs of cataract formation. M.H., a 52-year-old African American woman with brown eyes, presented for routine ophthalmic examination. Visual acuity without correction was 20/40 right eye and 20/80 left eye. M.H. related a positive family history for glaucoma and presently is being treated for hypertension, chronic heart failure (CHF), chronic obstructive pulmonary disease, and asthma. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 70. Her medications include the following: Amitriptyline, 75 mg at bedtime Chlorpheniramine, 4 mg every 6 hours as needed (PRN) Lisinopril, 10 mg once daily Furosemide, 40 mg BID Nitroglycerin, 0.3 mg sublingual PRN Fluticasone/salmeterol 250 mcg/50 mcg dry powder inhaler, one inhalation twice daily Albuterol 90 mcg metered-dose inhaler, 1-2 puffs QID PRN Tiotropium bromide inhaler, 18 mcg inhaled once daily Findings on examination indicate that M.H. has POAG. What other factors may predispose M.H. to an increased IOP? clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 71. 1. POAG is thought to be determined genetically, and M.H. has a positive family history. 2. The disease is more prevalent and aggressive in African Americans. 3. In addition, she is taking several medications that have been associated with increases in IOP. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 72. The IOP is always measured before this procedure, so the use of these agents would not have influenced the IOP readings in M.H. Anticholinergic Drugs Most reports dealing with drug-induced increases in IOP center around precipitation of angle-closure glaucoma by ophthalmic mydriatic or cycloplegic agents (anticholinergics). In patients with open-angle glaucoma, topical anticholinergics can significantly increase resistance to aqueous humor outflow As part of any routine ophthalmic examination, the pupils are dilated with a mydriatic or cycloplegic agent (unless otherwise contraindicated). clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 73. If systemic anticholinergic agents are administered in doses sufficient to cause pupillary dilation, the risk of precipitating angle-closure increases. these agents will aggravate open-angle glaucoma unless the amount reaching the eye is sufficient to cause cycloplegia. literature documentation of POAG exacerbation by these agents is scarce, medications with anticholinergic side effects should be considered. e.g.: 1. Antihistamines 2. Benzodiazepines 3. Disopyramide 4. Phenothiazines 5. Tricyclic antidepressants 6. Tiotropium clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 74. Therefore, it is highly unlikely that these medications contributed to her increased IOP M.H.is receiving: 1. Chlorpheniramine as needed 2. Amitriptyline at bed-time 3. Tiotropium bromide once daily but her pupil examination is normal with no evidence of mydriasis or cycloplegia. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 75. These have no proven adverse influences on IOP in patients with either normal eyes or eyes with open-angle glaucoma. Adrenergic Drugs Adrenergic agents may produce minimal pupillary dilation. , Such as : 1. Central nervous system stimulants 2. Vasoconstrictors 3. Appetite suppressants 4. Bronchodilators the use of salmeterol and albuterol in M.H. is also an unlikely source of the increased IOP. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 76. Other Drugs Conclusive evidence for the production of angle-closure glaucoma by vasodilators is lacking, although slight increases in IOP have been reported. Use of nitroglycerin as needed in M.H. is not a cause for concern. There have been isolated reports of other medications causing mydriasis in glaucoma patients.These include: 1. Muscle relaxants (carisoprodol) 2. Monoamine oxidase inhibitors 3. Fenfluramine 4. Ganglionic blocking agents 5. Salicylates 6. Oral contraceptives clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 77. Succinylcholine Ketamine Caffeine Have been associated with increases in IOP. If M.H. requires administration of any other medications associated with increases in IOP, the risk of potential adverse effects can be minimized by routine follow-up. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 78. CASE 1, QUESTION 2: What is the best initial therapeutic treatment in M.H.? Initial Therapy Topical β-blockers or PGAs are the initial agents of choice in the treatment of POAG . Their efficacy is well documented in numerous studies, and side effects are well characterized. Brimonidine (Alphagan) and Topical CAIS are alternative first-line agents. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 79. Betaxolol β1-adrenergic blocker better tolerated than the nonselective β- adrenergic blocker in patients with reactive airway disease should be considered when topical β-blocker therapy is indicated in patients such as M.H. Timolol or other nonselective β-adrenergic blockers should not be initiated for M.H. because of her history of asthma clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 80. Betaxolol 0.25% suspension BID would be reasonable for the initial treatment of M.H.’s glaucoma. adverse pulmonary and cardiac side effects can occur with betaxolol M.H. should be followed up closely for these adverse effects ocular burning and stinging have been associated more frequently with betaxolol and metipranolol than with other topical β-blockers the 0.25% suspension is better tolerated than the 0.5% solution and is as effective. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 81. Although brimonidine, topical CAIS, and latanoprost may not exacerbate her asthma or CHF They can cause localized side effects and Brimonidine can cause systemic hypotension and lethargy. Brimonidine, a topical CAI PGA (e.g.,latanoprost) Are acceptable alternatives to betaxolol as initial therapy. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 82. CASE 1, QUESTION 3: Betaxolol 0.25% suspension, one drop in both eyes BID, is ordered for M.H. How should M.H. be instructed regarding the proper use of her betaxolol and expected therapeutic side effects? rest that hand on her forehead to minimize the risk of inadvertent eye injury caused by sudden unexpected movement of the hand. M.H. should be instructed to hold the inverted betaxolol bottle between her thumb and middle finger 1 2 clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 83. The patient should look up and administer the drug into the pouch of the eye. The index finger is left free to depress the bottom of the container, releasing one drop for the dose. 3 The lower eyelid should be drawn downward with the index finger of the opposite hand or pinched between the thumb and index finger to form a pouch. 4 5 clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 84. Patients must be encouraged to continue regular use of their medications for effective treatment of glaucoma. Chronic glaucoma is a silent disease and often not associated with symptoms; therefore, the continuation of therapy should be encouraged continuously in patients, especially when side effects to drug therapy can be encountered. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 85. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary Betaxolol is best administered every 12 hours BECAUSE this schedule of administration is consistent with its duration of action. Systemic side effects are rare with betaxolol e.g.: 1. Bradycardia 2. heart block 3. CHF 4. pulmonary distress 5. central nervous system but M.H. should be instructed to report any of these effects to her primary-care provider.
- 86. CASE 1, QUESTION 4: How much would occlusion of the nasolacrimal ducts (punctal occlusion) by M.H. influence systemic absorption or alter the therapeutic effects of betaxolol? clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 Nasolacrimal, or punctal, occlusion is a technique that can decrease the amount of drug absorbed systemically. Nasolacrimal occlusion
- 87. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary Occlusion of the puncta (through the application of slight pressure with the finger to the inner corner of the eye closest to the nose for 3 to 5 minutes during and after drug instillation) 1. can minimize systemic absorption of ophthalmic medications (e.g.,betaxolol) 2. decrease the incidence of side effects 3. improve medication effectiveness.
- 88. When a single drop of ophthalmic timolol 0.5% was instilled into the eyes of patients at various times before cataract surgery and the nasolacrimal duct was occluded for 5 minutes, drug levels in the aqueous humor were significantly greater in patients who had their nasolacrimal ducts occluded than those who did not. The average measured maximal aqueous humor timolol concentration of 1.66 mcg/mL in the occlusion group was significantly greater than 0.85 mcg/mL in the non-occlusion group. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 The area under the curve was 1.7 times greater in patients who used the technique of naso-lacrimal occlusion, and the duration of action was prolonged.
- 89. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary Nasolacrimal occlusion Is effective and can maximize drug benefits Because a lower concentration of an ophthalmic formulation can be used the dose can be administered less frequently .
- 90. only 55% achieved comparable IOP reductions when nasolacrimal ducts were not occluded. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 Pilocarpine 1% and 2% significantly decreased IOP at 6, 8, and 12 hours after instillation when the technique of nasolacrimal occlusion was applied. Carbachol 1.5% and 3% The combination of carbachol 1.5% with timolol 0.25% every 12 hours Were maximally beneficial with nasolacrimal occlusion. reduced IOP by 15% maintained at 24 hours in 92% of patients when nasolacrimal occlusion was used Timolol
- 91. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary pilocarpine 2% and carbachol 1.5% can be administered every 12 hours rather than the usual TID or QID regimens needed Timolol can be administered every 24 hours if the nasolacrimal occlusion technique is used. maximal drug effect can be achieved with a reduced frequency of administration and at about half of the drug concentrations typically used. Nasolacrimal occlusion should be incorporated into patient counseling for instillation of all eye drops. When nasolacrimal occlusion is used
- 92. Alternative Therapy CASE -1, QUESTION 5: Two weeks after initiation of therapy M.H. returns to clinic for a follow-up evaluation. Her IOP measures 32 mm Hg in the right eye and 30 mm Hg in the left eye. She denies non-adherence and has no complaints of intolerable side effects. How should therapy be altered? Are there alternative dosage forms or drugs that can be used? Betaxolol may not be as effective as other ocular β-blockers. Therefore, adjunctive therapy may be required. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 93. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 M.H.should be evaluated to determine whether she has been using the technique of nasolacrimal occlusion M.H. should be again instructed on the technique of nasolacrimal occlusion and the importance of this technique in achieving the maximal therapeutic effect of her therapy If not, After the initiation of therapy, patients should be seen for a follow-up evaluation within about 2 weeks.
- 94. Patients who are experiencing unstable reductions of IOP should be followed up within 4 months. Stable patients usually are evaluated every 6 to 12 months. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 If M.H. has been adherent to therapy and has been occluding her nasolacrimal ducts a new course of action is needed because her IOP still is elevated When the goal of therapy has not been achieved 1. the drug concentration of the ophthalmic formulation can be increased 2. adjunctive therapy (e.g., brimonidine, a topical CAI, a PGA) can be initiated 3. an alternative first-line agent can be selected.
- 95. Adverse Effects CASE -1, QUESTION 6: Several weeks later dorzolamide 2% solution, one drop both eyes BID, is added to M.H.’s betaxolol therapy. Two weeks later, M.H. returns for a follow-up evaluation and complains of bilateral stinging and foreign body sensation. Her IOP measures 30 mm Hg in the right eye and 29 mm Hg in the left eye. What are the possible causes of her side effects and poor response to therapy? clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 96. 1-12-2016 clinical pharmacy department :Dr.Hemat Elgohary These granules can drop into a patient’s eyes when instilling the medication, leading to local side effects, such as stinging and foreign body sensation The exposure of dorzolamide to the outside environment may result in the aggregation of dry white granules on the tip of thedorzolamide bottle. Such foreign bodies may cause enough discomfort to induce non-adherence, resulting in a poor response to therapy. These granules may be rinsed off of the tip with sterile water. M.H. should be questioned about the presence of dry white granules on the tip of her dorzolamide bottle.
- 97. These complaints may also be a side effect from the medications, regardless of the granule presence. Ocular burning, stinging, and discomfort were reported in one- third of patients in dorzolamide clinical trials. M.H.’s administration technique should also be assessed to determine whether she is administering the two drugs at least 5 to 10 minutes apart so that the first drug is not washed away by the second drug. clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016 This should be a consideration when assessing her response to therapy.
- 98. CASE -1, QUESTION 7: After further discussions with M.H., it is determined that she has not been adherent to her dorzolamide therapy because of intolerable side effects. The dorzolamide is discontinued and replaced with travoprost 0.004% one drop both eyes once a day at bedtime. Why might this drug selection be especially appropriate for M.H.? What patient education information should be provided to M.H. about travoprost side effects? clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016
- 99. Prostaglandin analogs are first-line agents and are appropriate in patients who are not responding to or are having intolerable side effects from other medications. Travoprost is an ideal choice for M.H., because African Americans respond especially well to travoprost. M.H. still needs to be informed about the PGA- induced potential for hyperpigmentation of the iris, which may be permanent. She also needs to be educated on the possibility of eyelid skin darkening and increased thickness, length, and pigmentation of her eyelashes, which all may or may not be reversible. These side effects might not be as cosmetically concerning to M.H., because she has brown eyes and will be instilling travoprost eye drops into both eyes.clinical pharmacy department :Dr.Hemat Elgohary 1-12-2016