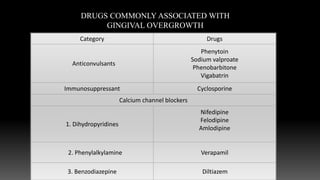
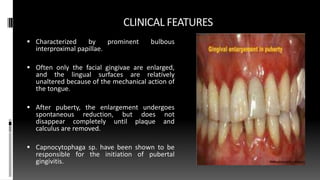
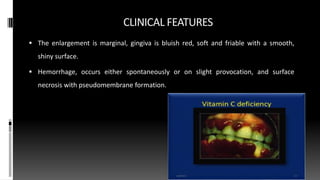
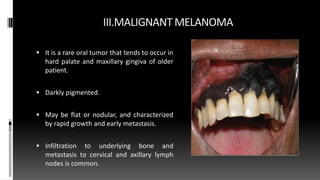
This document discusses gingival enlargement, classifying it as inflammatory, drug-induced, associated with systemic diseases or conditions, neoplastic, or false enlargement. Inflammatory enlargement includes chronic and acute types. Drug-induced enlargement is caused by medications like anticonvulsants, immunosuppressants, and calcium channel blockers. Enlargements can also be associated with conditions like pregnancy, puberty, or systemic diseases. Neoplastic enlargement refers to benign or malignant tumors of the gingiva. The document provides details on the clinical features, histopathology, grading, and pathogenesis of each type of gingival enlargement.




![Histological Classification [Barak in 1987]987)]
Grade I – Normal Gingiva - Width of epithelium - 0.3-0.5 mm.
Grade II – Slight Overgrowth - Width of epithelium 0.5-1.5 mm.
Grade III- Moderate Overgrowth –Width of epithelium 1.5-3 mm.
Grade IV – Severe Overgrowth- Width of epithelium 3- 4 mm.](https://image.slidesharecdn.com/gingivalenlargementppt-230718122048-33deef95/85/Gingival_enlargement_ppt-pptx-26-320.jpg)

































![GINGIVAL_ENLARGEMENT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gingivalenlargement1-230208043639-678d76d8-thumbnail.jpg?width=640&height=640&fit=bounds)

























































