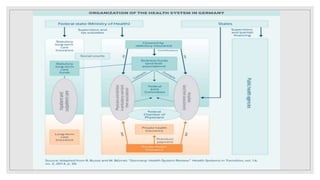
The document provides an overview of the German healthcare system. It describes how the system is based on both public and private insurance, with public insurance covering around 88% of the population. Public insurance is funded through income-related contributions from employers and employees. The system aims to provide equal coverage to all citizens regardless of income or age. It covers a wide range of medical services and utilizes various strategies to ensure quality of care and reduce disparities.