INTRODUCTION
• Anxiety canbe conceptualized as a
normal and adaptive response to threat
that prepares the organism for flight or
fight.
• Persons who seem to be anxious about
almost everything, however, are likely to
be classified as having generalized
anxiety disorder.
3.
• Generalized anxietydisorder is defined as
excessive anxiety and worry about several
events or activities for most days during
at least a 6-month period.
• The worry is difficult to control and is
associated with somatic symptoms, such
as muscle tension, irritability, difficulty
sleeping, and restlessness.
4.
• The anxietyis not focused on features of
another disorder
• is not caused by substance use or a general
medical condition
5.
• and doesnot occur only during a mood or
psychiatric disorder.
• The anxiety is difficult to control, is
subjectively distressing, and produces
impairment in important areas of a
person’s life.
6.
CLINICAL PICTURE
•Worry andapprehension that are more
prolonged than in healthy people.
•The worries are widespread and are not
focused on a specific issue as they are in panic
disorder (i.e. on having a panic attack), social
phobia (i.e. on being embarrassed), or OCD (i.e.
on contamination).
•The person feels that these widespread worries
are difficult to control.
7.
• Psychological arousal,which
may be manifested as
irritability, poor concentration,
and/or sensitivity to noise.
• Some patients complain of
poor memory, but this is
because of poor concentration.
• If true memory impairment is
found, a careful search should
be made for a cause other than
anxiety.
8.
Autonomic over-activity
• whichis most often experienced as sweating,
palpitations, dry mouth, epigastric discomfort, and
dizziness.
Muscle tension
• which may be experienced as restlessness, trembling,
inability to relax, headache (usually bilateral and frontal
or occipital), and aching of the shoulders and back.
9.
Hyperventilation
• which maylead to dizziness, tingling in
the extremities and, paradoxically, a
feeling of shortness of breath.
10.
Sleep disturbances
• difficultyin falling asleep and persistent
worrying thoughts.
• Sleep is often intermittent, unrefreshing,
and accompanied by unpleasant dreams.
• Some patients have night terrors and wake
suddenly feeling extremely anxious.
• Early-morning waking is not a feature of
GAD, and its presence strongly suggests a
depressive disorder.
11.
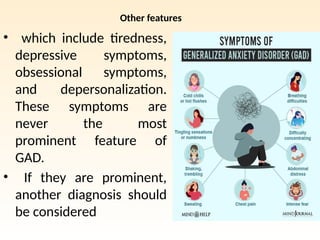
Other features
• whichinclude tiredness,
depressive symptoms,
obsessional symptoms,
and depersonalization.
These symptoms are
never the most
prominent feature of
GAD.
• If they are prominent,
another diagnosis should
be considered
12.
CLINICAL SIGNS
• Theface appears strained, the brow is
furrowed, and the posture is tense. The
person is restless and may tremble. The skin is
pale, and sweating is common, especially from
the hands, feet, and axillae. Being close to
tears, which may at first suggest depression,
reflects the generally apprehensive state.
13.
ICD10 DIGNOSTIC GUIDELINES
•The sufferer must have primary symptoms of anxiety
most days for at least several weeks at a time and
usually for several months. These symptoms should
usually involve elements of ;
In children, Frequent need for reassurance and recurrent
somatic complains may be prominent.
apprehension Motor tension Autonomic over-activity
worries about future
misfortunes. feeling “on
age”, Difficulty in
concentrating. Etc
restless fidgeting, tension
headaches ,Trembling ,
Inability to relax
lightheadedness,
Sweating , Tachycardia or
tachypnoea, Epigastric
discomfort, Dizziness. Dry
mouth, etc.
14.
COMORBIDITY
• Generalized anxietydisorder is probably the
disorder that most often coexists with another
mental disorder, usually social phobia, specific
phobia, panic disorder, or a depressive disorder.
• Perhaps 50 to 90 percent of patients with
generalized anxiety disorder have another
mental disorder.
• As many as 25 percent of patients eventually
experience panic disorder.
15.
• An additionalhigh percentage of patients
are likely to have major depressive
disorder.
• Other common disorders associated
with generalized anxiety disorder are
dysthymic disorder and substance
related disorders
16.
EPIDEMIOLOGY
• The AdultPsychiatric Morbidity Survey
found a 12-month prevalence of 4.4% for
GAD in England .
• a similar figure has been reported in US
surveys, with rather lower prevalence
figures in European countries (around 2%;
Wittchen et al., 2011).
• Rates in women are about twice as high as
those in men.
17.
Prevalence of anxietydisorders in India
• Reddy and Chandrashekhar, in their meta-analysis of
13 studies with a sample size of 33 572 subjects,
found neurotic disorders to have the highest
estimated prevalence rate, 20.7% (18.7% to 22.7%).
Of the neurotic disorders they studied, only phobia
and GAD are included under anxiety disorders as
per the current DSM-5 criteria, with weighted
prevalence values of 4.2% and 5.8% respectively.
• Urban communities had higher prevalence rates
(35.7% vs 13.9%) than rural communities.
18.
• GAD isassociated with several indices of
social disadvantage, including lower
household income and unemployment, as
well as divorce and separation (McManus
et al., 2009).
• Rates of anxiety, as well as expressions of
anxiety, vary across development, and the
anxiety disorders are the most common
child mental disorders
19.
AETIOLOGY
In general terms,
•GAD appears to be
caused by stressors
acting on a personality
that is predisposed to
anxiety by a combination
of genetic factors and
environmental
influences in childhood.
20.
Stressful events
• Astudy by Kendler et al. (2003) showed that
stressful life events characterized by loss
increased the risk of both depression and
GAD. However, life events characterized by
‘danger’ (where the full import of the event
was yet to be realized) were more common in
those who subsequently developed GAD.
21.
Genetic causes
• Earlytwin studies, such as that by Slater and
Shields (1969), showed a higher concordance
for anxiety disorder between monozygotic
than dizygotic pairs, which suggests that the
familial association has a genetic cause.
• However, the genes involved in the
transmission of GAD appear to increase
susceptibility to other anxiety conditions, such
as panic disorder and agoraphobia, as well as to
major depression.
22.
• Overall, thefindings suggest that genes play a
significant although moderate role in the
aetiology of GAD, but that the genes involved
predispose to a range of anxiety and
depressive disorders, rather than GAD
specifically (Shimada-Sugimoto et al., 2015).
23.
Social Factors
• Brownand Harris (1993) studied the
relationship between adverse experience in
childhood and anxiety disorder in adult life in
404 working-class women living in an inner
city.
• Adverse early experience was assessed from
patients’ accounts of parental indifference and
of physical or sexual abuse.
24.
• Women whoreported early adversity
had increased rates of GAD (and also
of agoraphobia and depressive
disorder, but not of simple phobia).
25.
Parenting styles
• characterizedby overprotection and lack of
emotional warmth may also be a risk factor for
GAD, as well as for other anxiety and
depressive disorders in offspring.
Early experiences
• Accountsgiven by anxious patients of
their experience in childhood suggest
that early adverse experience is a cause
of GAD. These accounts have given rise
to objective studies and to
psychoanalytic theories.
• the outside world (realistic anxiety);
• the instinctual levels of the id, including
love, anger, and sex (neurotic anxiety);
28.
THE SUPEREGO (moralanxiety)
• According to this theory, in GAD, anxiety
is experienced directly unmodified by the
defence mechanisms that are thought to
be the basis of phobias or obsessions.
• The theory proposes that in GADs the
ego is readily overwhelmed because it has
been weakened by a development failure
in childhood.
29.
• Normally, childrenovercome this anxiety
through secure relationships with loving
parents.
• However, if they do not achieve this
security, as adults they will be vulnerable
to anxiety when experiencing separation
or potentially threatening events.
30.
• Thus bothpsychoanalytic ideas and
objective studies suggest that good
parenting can protect against anxiety by
giving the child a secure emotional base
from which to explore an uncertain world
31.
Cognitive Behavioural Theory
•Conditioning theories propose that GAD arises
when there is an inherited predisposition to
excessive responsiveness of the autonomic
nervous system, together with generalization of
the responses through conditioning of anxiety
to previously neutral stimuli.
32.
• This theoryhas not been supported by a
body of objective data.
• Cognitive theory. Particular coping and
cognitive styles may also predispose
individuals to the development of GAD,
33.
• it seemslikely that people who lack a sense of
control of events and of personal
effectiveness, perhaps because of early life
experiences, are more prone to anxiety
disorders.
• Such individuals may also demonstrate trait-
like cognitive biases in the form of increased
attention to potentially threatening stimuli,
overestimation of environmental threat, and
enhanced memory of threatening material.
34.
• More recentcognitive formulations have focused on
the process of worry itself. It has been proposed
that people who are predisposed to GAD use worry
as a positive coping strategy for dealing with
potential threats,
• whereby the individual cannot relax until they have
examined all of the possible dangers and identified
ways of dealing with them.
35.
• However, thiscan lead to ‘worry about worry’,
when a person comes to believe, for example,
that worrying in this way, although necessary for
them, is also uncontrollable and harmful.
• This ‘metacognitive belief’ may form a transition
between excessive but normal worrying, and
GAD (Wells, 2013)
36.
Personality
• Anxiety symptomsare associated with
neuroticism, and twin studies have shown
an overlap between the genetic factors
related to neuroticism and those related to
GAD (Hettema et al., 2004).
37.
Personality disorder
• GADoccurs in people with anxious–avoidant
personality disorders, but also in individuals
with other personality disorders
38.
Neurobiological mechanism
• Studiesin animals have indicated a key role for
the amygdala, which receives sensory
information both directly from the thalamus
and from a longer pathway involving the
somatosensory cortex and anterior cingulate
cortex.
• Cortical involvement in anxiety is important
because it indicates a role for cognitive
processes in its expression.
39.
• The hippocampusis also believed to have an
important role in the regulation of anxiety,
because it relates fearful memories to relevant
present contexts.
• Breakdown of this mechanism could lead to an
overgeneralization of fear in response to
nonthreatening stimuli (Cain et al., 2013).
40.
Animal experimental
• studieshave led to an understanding of the
regulation of anxiety in the brain by
neurotransmitters and neuromodulators.
• Noradrenergic neurons that originate in the locus
coeruleus increase arousal and anxiety,
• whereas 5-HT neurons that arise in the raphe
nuclei appear to have complex effects, and serve
both to signal the presence of anxiety-producing
stimuli in the environment and also to restrain the
associated behavioral responses.
41.
(GABA)
• Gamma-aminobutyric acidreceptors, which
are widely distributed in the brain, are
inhibitory and reduce anxiety, as do the
associated benzodiazepine-binding sites.
42.
• There isprobably also an important role for
corticotropin-releasing hormone, which increases
anxiety-related behaviours and is found in high
concentration in the amygdala.
• However, although pharmacological manipulation
of 5-HT and GABA mechanisms can be helpful in
the treatment of generalized anxiety, there is no
firm evidence that changes in these
neurotransmitters are fundamentally involved in
the pathophysiology of the disorder (Garner
et al., 2009).
43.
• Functional imagingof the brain during the
presentation of aversive stimuli (e.g. fearful
faces) has shown inconsistent changes in
amygdala reactivity in patients with GAD.
• There is more reliable evidence of altered
activity in cortical regulatory regions such as
the ventrolateral prefrontal cortex and
altered connectivity between this region
and the amygdala
44.
Differential diagnosis
• GADhas to be distinguished not only from
other psychiatric disorders but also from
certain physical conditions.
• Anxiety symptoms can occur in nearly all
psychiatric disorders, but there are some in
which particular diagnostic difficulties arise.
45.
Depressive disorder
• Anxietyis a common symptom in
depressive disorder, and GAD often
includes some depressive symptoms.
• The usual convention is that the diagnosis
is decided on the basis of the severity of
two kinds of symptom and the order in
which they appeared
46.
Information on thesetwo points should be
obtained, if possible, from a relative or other
informant as well as from the patient.
Whichever type of symptoms appeared first and is
more severe is considered primary.
47.
An important diagnosticerror is to misdiagnose
the agitated type of severe depressive disorder as
GAD.
This mistake will seldom be made if anxious
patients are asked routinely about symptoms of a
depressive disorder, including depressive thinking
and, when appropriate, suicidal ideas.
As noted above, in some patients a depressive
disorder and GAD coexist and both diagnoses can
be made
48.
Schizophrenia
• People withschizophrenia sometimes complain of
anxiety before the other symptoms are recognized.
• The chance of misdiagnosis can be reduced by asking
anxious patients routinely what they think caused their
symptoms.
• Schizophrenic patients may give an unusual reply,
which leads to the discovery of previously unexpressed
delusional ideas.
49.
Dementia
• Anxiety maybe the first abnormality to be
complained of by a person developing
dementia.
• When this happens, the clinician may not
detect an associated impairment of memory, or
may dismiss it as the result of poor
concentration. Therefore memory should be
assessed in middle-aged or older patients who
present with anxiety.
50.
Substance Misuse
• Somepeople take drugs or alcohol to relieve
anxiety.
• Patients who are dependent on drugs or
alcohol sometimes believe that the symptoms
of drug withdrawal are those of anxiety, and
take anxiolytic or other drugs to control them.
• The clinician should be alert to this possibility,
particularly when anxiety is severe on waking in
the morning, which is the time when alcohol
and drug withdrawal symptoms tend to occur.
51.
Prognosis
• One ofthe DSM-5 criteria for GAD is that the
symptoms should have been present for 6 months.
• One of the reasons for this cut-off is that anxiety
disorders that last for longer than 6 months have a
poor prognosis.
52.
• Thus mostclinical studies suggest that
GAD is typically a chronic condition with
low rates of remission over the short and
medium term.
• Evaluation of the prognosis is complicated
by the frequent comorbidity with other
anxiety disorders and depression, which
worsen the long-term outcome and
accompanying burden of disability
53.
• In theHarvard–Brown Anxiety Research
Program, which recruited patients from Boston
hospitals, the mean age of onset of GAD was
21 years, although many patients had been
unwell since their teenage years.
• The average duration of illness in this group
was about 20 years and, despite treatment, the
outcome over the next 3 years was relatively
poor, with only one in four patients showing
symptomatic remission from GAD (Yonkers
et al., 1996).
54.
• However, theparticipants in the above study
were recruited from hospital services, and
may not be representative of GAD in
community settings.
• In a naturalistic study in the UK, Tyrer and
colleagues (2004a) followed up patients with
anxiety and identified in primary care and
found that, 12 years later, 40% of those
initially diagnosed with GAD had recovered, in
the sense that they no longer met the criteria
for any DSM-III psychiatric disorder.
55.
• The remainingparticipants continued to be
symptomatic, but in only 3% was GAD still the
principal diagnosis. In the vast majority of
patients, conditions such as dysthymia, major
depression, and agoraphobia were now more
prominent.
• This study confirms the chronic and fluctuating
symptomatic course of GAD in many clinically
identified patients
56.
TREATMENT
• SELF-HELP ANDPSYCHOEDUCATION - A variety of
forms of self-help have been studied in patients
with anxiety disorders, including GAD.
• Such approaches typically include written and
electronic materials with information about the
disorder, and practical exercises to carry out based
on the principles of cognitive behaviourl therapy.
57.
• Typically self-helphas minimal therapist
input.
• but it is also possible for self-help for anxiety
disorders to be guided by a trained
practitioner (guided self-help).
58.
GROUP PSYCHOEDUCATION
• whereone therapist works with up to a dozen
clients in about six weekly sessions of
interactive learning and shared experience.
• The evidence for the benefit of these forms
of treatment is limited and the effects,
although superior to no treatment, appear to
be modest.
• However, these approaches are useful as part
of an initial stepped-care approach.
59.
RELAXATION TRAINING
• Ifpractised regularly, relaxation appears to be
able to reduce anxiety in less severe cases.
• However, many patients with such disorders do
not practise the relaxation exercises regularly.
• Motivation may be improved if the training
takes place in a group, and some people engage
more with treatment when relaxation is taught
as part of a programme of yoga exercises.
60.
• A structuredtherapy, known as applied
relaxation, does appear to be effective in
lowering anxiety over 12–15 sessions
guided by a trained therapist (Hoyer et
al., 2009).
• A critical element of this treatment is the
application of learned relaxation skills to
anxiety-provoking situation
61.
Cognitive behaviour therapy
•This treatment combines relaxation with
cognitive procedures designed to help
patients to control worrying thoughts.
• Compared with treatment as usual,
cognitive behaviour therapy produces quite
substantial benefits in terms of symptom
resolution, with relatively few dropouts.
62.
• However, theoutcome obtained with
cognitive therapy does not appear to differ
from that obtained with other kinds of
psychological interventions, such as
applied relaxation and non-directive
counselling, and there are few data on
longer-term outcomes.
63.
Medication
• Medication canbe used to bring symptoms
under control quickly while the effects of
psychological treatment are awaited.
• It can also be used when psychological treatment
has failed.
64.
• However, medicationis often prescribed too
readily and for too long.
• Before prescribing, it is appropriate to recall
that, even though GAD is said to have a poor
prognosis, in short-term studies of medication,
pill placebo treatment in the context of the
clinical care provided by a controlled trial is
beneficial for a significant proportion of patients.
65.
• For example,in a 12-week, placebo-controlled
trial of escitalopram and paroxetine, just over
40% of patients responded to placebo, and
around 30% reached remission .
66.
Short-term treatment
• Oneof the longer-acting benzodiazepines, such
as diazepam, is appropriate for the short-term
treatment of GADs—for example, diazepam in a
dose ranging from 5 mg twice-daily in mild
cases to 10 mg three times daily in the most
severe cases.
• Anxiolytic drugs should seldom be prescribed
for more than 3 weeks, because of the risk of
dependence when they are given for longer.
67.
• Buspirone issimilarly effective for short-term
management of GAD and is less likely to cause
dependency, but has a slower onset of action.
• Betaadrenergic antagonists are sometimes
used to control anxiety associated with
sympathetic stimulation.
• However, they are more often used for
performance anxiety than for GAD.
68.
Long-term treatment
• BecauseGAD often requires lengthy
treatment, for which benzodiazepines are
unsuitable (see above), and is often comorbid
with depression and other anxiety disorders,
treatment guidelines usually recommend
69.
• selective serotoninreuptake inhibitors
(SSRIs) as the initial choice,
• Serotonin and noradrenaline reuptake
inhibitors (SNRIs) such as duloxetine and
venlafaxine are also effective, but are
somewhat less well tolerated than SSRIs.
70.
• The anticonvulsantpregabalin is also
licensed for the treatment of GAD in the
UK.
• It has a different side effect profile to
SSRIs and SNRIs, and might therefore be
useful in patients who cannot tolerate the
latter agents.
71.
• Where patientswith GAD respond to
medication, the risk of relapse is substantially
reduced if treatment is maintained for at least 6
months, and probably longer.