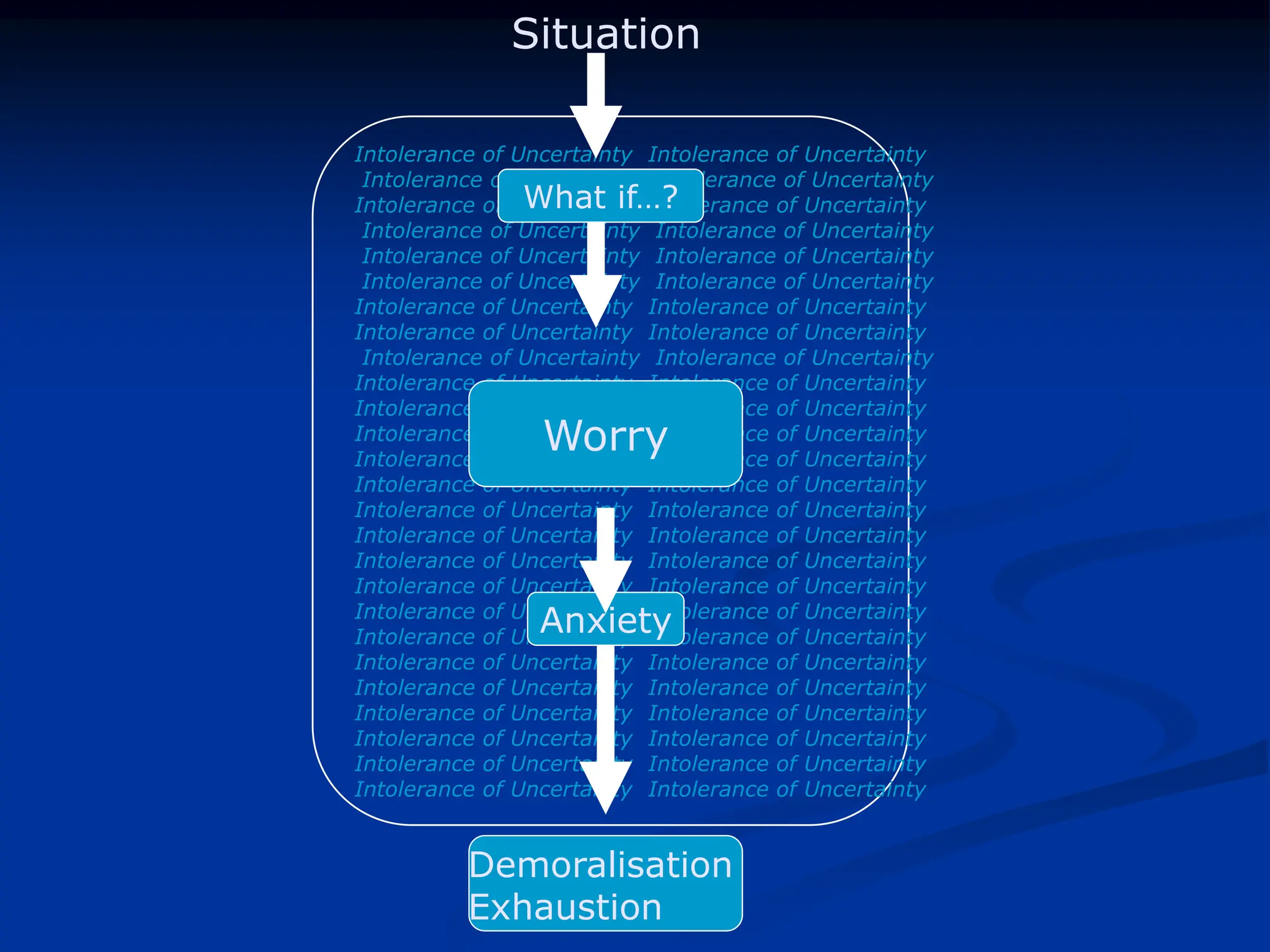
Generalized anxiety disorder (GAD) affects 3-8% of the population with a higher prevalence in women and significant comorbidity with other psychiatric disorders, particularly depression and other anxiety disorders. GAD is characterized by excessive anxiety and worry lasting at least six months, leading to various physical and emotional symptoms such as muscle tension, irritability, and sleep disturbances, with chronicity and low remission rates reported. Treatment through cognitive behavioral therapy (CBT) has shown moderate to large improvements, with a focus on managing worry and addressing the intolerance of uncertainty.