Downloaded 73 times
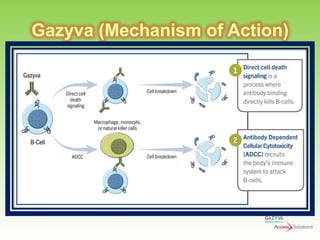
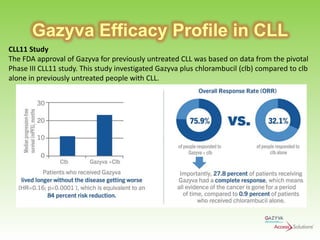
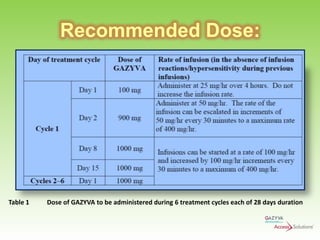
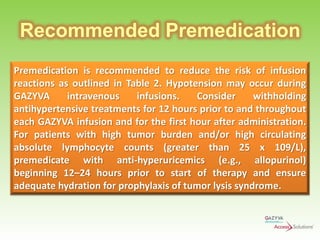
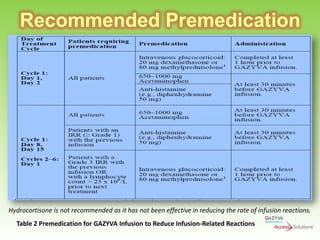

Gazyva (obinutuzumab) is a humanized anti-CD20 monoclonal antibody used for treating previously untreated chronic lymphocytic leukemia (CLL) in combination with chlorambucil chemotherapy. The drug targets CD20 on B-cells and has shown to improve survival without disease progression compared to chlorambucil alone in clinical trials. Administration requires careful premedication and monitoring due to potential severe infusion reactions.


































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















