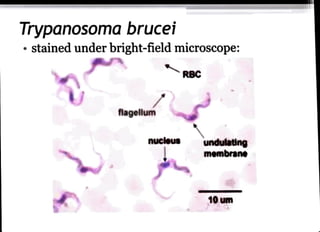
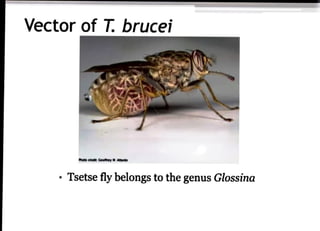
The document discusses Entamoeba histolytica and Trypanosoma species, focusing on their morphology, life cycles, and the diseases they cause, namely amoebiasis and Chagas disease. E. histolytica is prevalent in poor sanitary conditions, primarily affecting the large intestine and causing symptoms like amoebic dysentery, while T. brucei and T. cruzi are transmitted by tsetse flies and reduviid bugs, respectively, leading to serious conditions such as sleeping sickness and Chagas disease. Diagnosis and treatment methods for these parasitic infections are also outlined, emphasizing the importance of early intervention and preventive measures.















![Entamoeba_histolytica[1].pptparasitology](https://cdn.slidesharecdn.com/ss_thumbnails/entamoebahistolytica1-251110165959-534d5627-thumbnail.jpg?width=640&height=640&fit=bounds)














































