This document outlines Lori Dixon's program of study and professional development plan for a Master of Science in Nursing degree with a specialization in nursing informatics. It provides background on her nursing career spanning over 25 years, from becoming a registered nurse to her current role in clinical informatics. It describes her motivation to further her education to make more of an impact on patient care through her informatics work. The plan details the courses she will take to complete the degree and her goals of gaining skills in APA writing style and critically reviewing research to support her work in clinical trials and research.













![Developing a Health Advocacy Campaign
Nurses have an ethical responsibility to be active in advocacy. Nurses should address
issues with populations, and speak out to make changes in disparities or inequities to access to
care (Laureate Education, Inc. [Laureate], 2012). The purpose of this paper is to describe a
population health issue, identify the population it affects, review current health advocacy
programs and develop a health advocacy program.
Population Health Issue
The Affordable Care Act (ACA) is designed to provide healthcare for all Americans.
The emphasis is “all Americans.” To be eligible for care, an immigrant must have legal
immigrant status ("ACA Latinos," 2014). Migrant workers in the United States are a mixture of
legal and illegal workers. There are nearly a million farm workers, and 25-50% are illegal
immigrants (Baragona, 2010). Farm workers have families that travel with them from state to
state.
Patients go to a new provider, and the first thing that happens is the collection of their
health history. The new provider may ask for a release to get medical records from a previous
provider. Illegal or legal migrants move so frequently that they do not have a primary health
care provider. They may seek emergency or urgent care when they become ill, and children may
not receive important check-ups. There are barriers to healthcare such as unable to speak
English, the cost of care, availability of care, and distrust of healthcare workers. Hispanic
workers have health issues such as diabetes, sexually transmitted disease, teenage pregnancy,
and cirrhosis (Peach, 2013). The health issue is a lack of healthcare due to barriers that prevent
migrant workers and their families from receiving consistent healthcare. By traveling from state
to state, there is no history of their medical care for new providers to review.](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-17-320.jpg)




![Laureate Education, Inc. (Producer). (2012,). The needle exchange program [Interview
transcript]. Retrieved from
https://class.waldenu.edu/webapps/portal/frameset.jsp?tab_tab_group_id=_2_1&url=%2
F
webapps%2Fblackboard%2Fexecute%2Flauncher%3Ftype%3DCourse%26id%3D_5100
419_1%26url%3D
Mulligan, R., Seirawan, H., & Faust, S. (2010, February). Oral health care delivery model for
underserved migrant children. Journal of the California Dental Association, 38, 115-121.
Retrieved from http://www.cda.org/
National Center for Farmworker Health website. (2014). http://www.ncfh.org/
National Immigration Center website. (n.d.). http://www.nilc.org/
Peach, H. (2013, May 3). Migrant farm-workers and health. Rural and Remote Health, 13, 1-3.
Retrieved from http://www.rrh.org.au
The Affordable Care Act and Latinos. (2014). Retrieved from
http://www.hhs.gov/healthcare/facts/factsheets/2012/04/aca-and-latinos04102012a.html
The legislative Process. (2011). Retrieved from http://congress.indiana.edu/legislative-process
Waldeman, H. B., Cannella, D., & Perlman, S. P. (2010, November). Migrant farm workers and
their children. Exceptional Parent, 52-53. Retrieved from www.eparent.com](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-25-320.jpg)




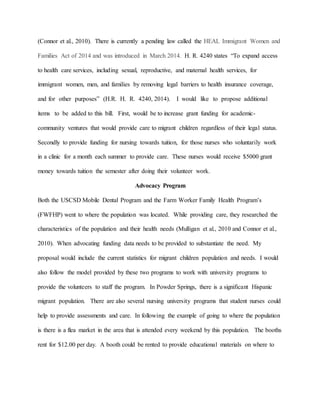
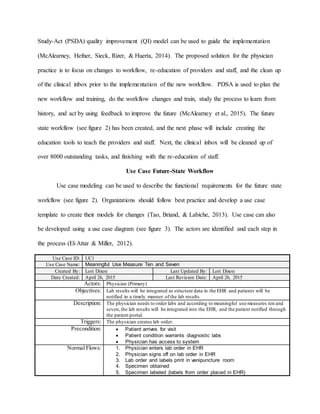
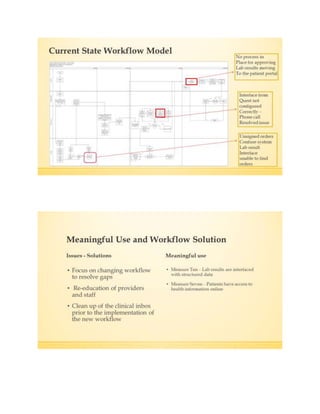
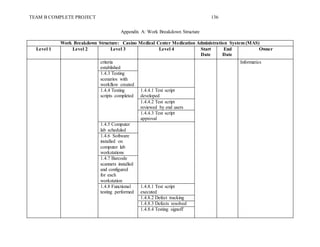
![the results tab in SCM for the physician’s review. The nurse notifies the physician that the
patient is ready to be seen.
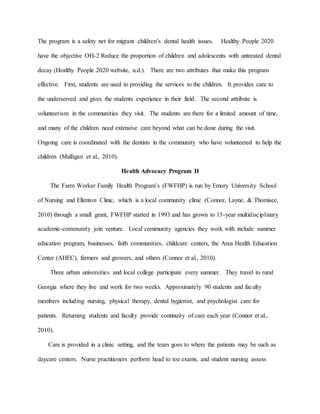
Pre-Infusion Physician Process
Page two in the process flow focuses around the physician’s visit with the patient. Prior to
going into the patient’s room, reviews the patient’s lab results to prepare for discussing treatment
options with the patient. If the patient’s Hemoglobin (Hb) ≤11 g/dL or ≥2 g/dL below baseline,
the patient may need a transfusion prior chemotherapy (NCCN Guidelines Version 2.2015 Panel
Members Cancer- and Chemotherapy-Induced Anemia [NCCN Panel], 2014). The flow chart
shows the decision point for no; and the chemotherapy cannot be given, and treatment for anemia
will begin. Or the decision is yes, because the labs show the patient values are within range, and
they can proceed with chemotherapy. The physician will open the progress note, and pull the
labs into the note and notate they have reviewed the labs with the patient. Next the physician
will open ORM through the progress note and review the medications with the patient. The
physician will reconcile the medications, and make any prescription changes needed ("TJC
Patient Safety," 2014). The physician will review the previous chemotherapy administered to the
patient in the treatment summary in SCM. Patient should receive the same chemotherapy dosing
unless there are changes in the patient’s condition. The physician will now order the
chemotherapy protocol for the patient. The nurse now escorts the patient to scheduling to review
the schedule for the week. Schedulers will review with the patient in ES, and the patient can
come anytime during the next day, and scheduler will make changes based on the patient’s
needs. The patient will now proceed to the infusion center.](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-33-320.jpg)


![References
AHRQ Agency for Healthcare Research and Quality. (2013). http://healthit.ahrq.gov/health-it-
tools-and-resources/
Morgenstern, D. (n.d.). Clinical workflow analysis - Process defect identification [PowerPoint
slides]. Retrieved from
http://mehi.masstech.org/sites/mehi/files/documents/CPOE_Clinical_Workflow_Analysis
.pdf
NCCN Guidelines Version 2.2015 Panel Members Cancer- and Chemotherapy-Induced Anemia.
(2014). Cancer -and chemotherapy - induced anemia. Retrieved from
http://www.nccn.org/professionals/physician_gls/pdf/anemia.pdf
National Patient Safety Goals Effective January 1, 2014. (2014). Retrieved from
http://www.jointcommission.org/assets/1/6/HAP_NPSG_Chapter_2014.pdf
Neuss, M. N., Polovich, M., McNiff, K., Esper, P., Gilmore, T. R., LeFebvre, K. B., Jacobson, J.
O. (2013, March). 2013 Updated American Society of Clinical Oncology/Oncology
Nursing Society Chemotherapy administration safety standards including standards for
the safe administration and management of oral chemotherapy [Supplemental material to
magazine]. Journal Of Oncology Practice, 5s-13s. doi: 10.1200/JOP.2013.000874](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-37-320.jpg)


![4. Does the documentation in the patient chart provide the data necessary for quality
indicators?
5. Do the physicians need education on documentation in the patient’s chart? What is
the definition of appropriate documentation?
The issue is that the documentation is not supporting the quality indicators or financial
reimbursement. Each of the questions above is background questions, they each look at a piece
of the issue but would not be complete enough to answer the clinical question.
Feasibility
Once the problem is identified for research, the researcher must decide if it is feasible to
research the problem. The following areas must be reviewed, although they may not be
necessary for every research study; time, participant availability, cooperation of others,
equipment, facilities, money, and ability of the researcher (Polit & Beck, 2012). Facilities and
providers will be forced into the ICD-10 changes on October 1, 2015. To provide evidence-
based change in the facility, it is necessary to create a research plan that would take place over
six months. The facility is willing to cooperate with the research plan, and minimal funding will
be needed. Two units will be identified to be part of the study, one will be a control group that
will not have a CDIP assigned to the unit, and the other unit will have a CDIP to educate the
physicians. The participants will be the hospitalists that are assigned to each unit, and the units
selected each uses a different group of hospitalist (Polit & Beck, 2012). The researcher is a
certified CDIP, who has passed their certification exam through the American Health
Information Management Association (AHIMA) (American Health Information Management
Association [AHIMA], n.d.). The current electronic health record (EHR) will be used for the
chart reviews, and the facility will grant the researcher access to the EHR.](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-41-320.jpg)




![References
American Health Information Management Association. (n.d.). Certified documentation
improvement practitioner (CDIP®). Retrieved from http://www.ahima.org/
Battelle. (2011). Quality indicator user guide: Patient safety indicators (PSI) composite
measures V4.3. Retrieved from
http://qualityindicators.ahrq.gov/downloads/modules/psi/v43/composite_user_technical_s
pecification_psi_4.3.pdf
Brown, L. R. (2013). The secret life of a clinical documentation improvement specialist
[Supplemental material]. Nursing, 10-12. doi: 10.1097/01.NURSE.
0000426541.97687.87.
Byrnes, J., & Fifer, J. (2010). A guide to highly effective quality programs. Healthcare financial
Management, 81-87. Retrieved from hfma.org
Carman, M. J., Wolf, L. A., Henderson, D., Kamienski, M., Koziol-McLain, J., Manton, A., &
Moon, M. D. (2013). Developing your clinical question: The key to successful research.
Journal of Emergency Nursing, 39, 299-301. doi: 10.1016/j.jen.2013.01.011
Hinderks, J., Vagle, J., & Wolf, J. (2014). Preparing for the true risks of ICD-10. Healthcare
Financial Management, 98-102. Retrieved from hfm.org
Hines, P. A., & Yu, K. M. (2009). The changing reimbursement landscape: Nurses’ role in
quality and operational excellence. Nursing Economic$, 27, 7-14. Retrieved from
https://www.nursingeconomics.net/
Kealey, B., & Howie, A. (2013, November). ICD-10 is coming: An update on medical diagnosis
and inpatient procedure coding. Minnesota Medicine, 48-50. Retrieved from
www.minnesotamedicine.com/_](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-51-320.jpg)
![Larkin, H. (2012, November). Focus on the c-suite: listener-in-chief. Hospitals & Health
Networks, 32-36. Retrieved from www.hhnmag.com
McDonald, K. M., Matesic, B., Contopoulos-loannidis, D. G., Lonhart, J., & Schmidt, E. (2013).
Patient safety strategies targets at diagnostic errors [Supplemental material]. Annals of
Internal Medicine, 158(5), 381-389. doi: 10.7326/0003-4819-158-5-201303051-00004
Michalak, J. (2011). The quality of patients’ data in medical documentation and statistical forms.
Studies in logic, grammar and rhetoric, 25(38), 143–158. Retrieved from
http://journals.indexcopernicus.com
Nichols, J. C. (2014, November 15). ICD-10 and clinical documentation [Video file]. Retrieved
from http://www.medscape.org/
Polit, D. F., & Beck, C. T. (2012). Nursing Research Generating and assessing evidence for
nursing practice (9th ed.). Philadelphia, PA: Wolters Kluwer Lippincott Williams &
Wilkins.
Quan, H., Eastwood, C., Cunningham, C., Liu, M., Flemons, W., De Coster, C., & Ghali, W. A.
(2013). Validity of AHRQ patient safety indicators derived from ICD-10 hospital
discharge abstract data (chart review study). British Medical Journal Open, 3, 1-7. doi:
10.1136/bmjopen-2013-003716
Richardson, A., & Storr, J. (2010). Patient safety: a literature review on the impact of nursing
empowerment, leadership and collaboration. International Nursing Review, 57, 12-21.
Retrieved from http://www.icn.ch/
Riva, J. J., Malik, K. M., Burnie, S. J., Endicott, A. R., & Busse, J. W. (2012). What is your
research question? An introduction to the PICOT format for clinicians. Journal of the](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-52-320.jpg)


![55
Planned Change in a Department
To Err is Human: Building a safer health system reports that medication errors are
occurring frequently, even with technology in place to make medication administration safer
(Committee on quality of health care in America [IOM Committee], 1999). Nursing leaders
have a responsibility to lead changes within a department or across departments. The purpose of
this paper is to review the issue in a department, describe how to change practice to meet facility
mission, vision, values, and professional standards. Describe how to facilitate the change using a
change model, and the stakeholders who should be involved.
Problem in the Department
The patient had stopped the nurse before the chemotherapy was administered, to let the
nurse know that this was not the chemotherapy she should receive. A review was done based on
this episode for the number of chemotherapy errors in the last six months. Chemotherapy
administration involves intricate protocols with high-risk medications. The size of the error can
determine how harmful it could be to the patient. Even a small error could cause renal damage
(Vioral & Kennihan, 2012). The risk management department completed the review, and they
found an average of 30 chemotherapy errors per month. The errors were primarily wrong drug
and wrong dose.
Specific Change to Practice
The policy at the hospital stated that two nurses had to verify the “Five Rights” of
medication administration at the patient bedside. The American Society of Clinical Oncology
(ASCO) and Oncology Nurse Society (ONS) standards state “A practitioner who is
administering the chemotherapy confirms with the patient his/her planned treatment prior to each](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-55-320.jpg)

![References
Committee on quality of health care in America. (1999). To err is human: Building a safer health
system [Issue brief]. Retrieved from Institute of Medicine website: http://www.iom.edu
Cancer Treatment Centers of America website. (n.d.). http://www.cancercenter.com
Code of Ethics for Nurses. (2010). Retrieved September 21, 2014, from
http://www.nursingworld.org
Marquis, B. I., & Huston, C. J. (2012). Leadership Roles and Management Functions in Nursing
(7th ed.). Philadelphia, PA: Wolters Kluwer Lippincott Williams & Wilkins.
Neuss, M. N., Polovich, M., McNiff, K., Espir, P., Gilmore, T. R., LeFebvre, K. B., ... Jacobson,
J. O. (2013, March). 2013 Updated American Society of Clinical Oncology/Oncology
Nursing Society Chemotherapy Administration Safety Standards including standards for
the safe administration and management of oral chemotherapy. JOURNAL OF
ONCOLOGY PRACTICE, 9(2s), 5s-13s. doi: 10.1200/JOP.2013.000874
Vioral, A. N., & Kennihan, H. K. (2012, December). Implementation of the American Society of
Clinical Oncology and Oncology Nursing Society Chemotherapy Safety Standards: A
multidisciplinary approach. Clinical Journal of Oncology Nursing, 16, E226-E230. doi:
10.1188/12.CJON.E226-E230](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-60-320.jpg)























































![References
American Nurses Association. (2008). Nursing informatics : scope and standards of practice.
Silver Spring, Md.: American Nurses Association.
Aveyard, H. (2007). Doing a literature review in health and social care: A practical guide:
McGraw-Hill International [UK] Limited.
Berner, E. S. (2008). Ethical and legal issues in the use of health information technology to
improve patient safety. HEC Forum: An Interdisciplinary Journal On Hospitals' Ethical
And Legal Issues, 20(3), 243-258. doi: 10.1007/s10730-008-9074-5
Bonkowski, J., Carnes, C., Melucci, J., Mirtallo, J., Prier, B., Reichert, E., . . . Weber, R. (2013).
Effect of Barcode-assisted Medication Administration on Emergency Department
Medication Errors. Academic Emergency Medicine, 20(8), 801-806. doi:
10.1111/acem.12189
Cork, R. D., Detmer, W. M., & Friedman, C. P. (1998). Development and Initial Validation of an
Instrument to Measure Physicians' Use of, Knowledge about, and Attitudes Toward
Computers (Vol. 5).
Frame the boundaries for an evaluation. (2013). Retrieved July 20, 2015, from
http://betterevaluation.org/plan/engage_frame/criteria_and_standards
Friedman, C. P., & Wyatt, J. C. (2006a). Developing and improving measurement methods
Evaluation Methods in Biomedical Informatics (pp. 145-187). New York, NY: Springer,
NY.
Friedman, C. P., & Wyatt, J. C. (2006b). Evaluation as a field Evaluation Methods in Biomedical
Informatic (pp. 21-47). New York, NY: Springer New York.](https://image.slidesharecdn.com/4b8d9c7d-55a0-4705-8f5f-53f25e3bcf63-151104213538-lva1-app6891/85/FinalPortfolioDraft-September-1-2015-154-320.jpg)