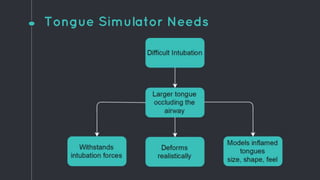
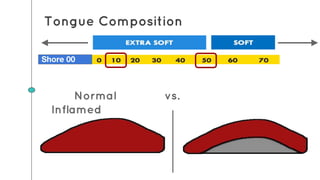
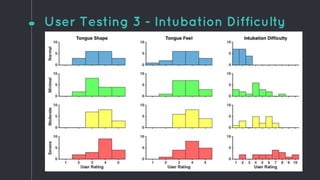
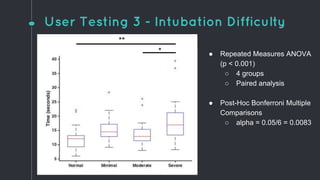
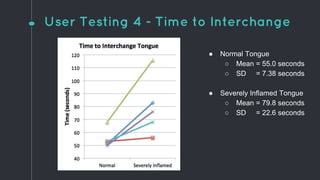
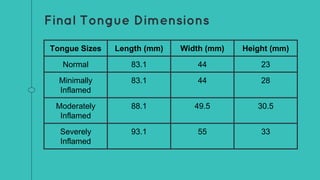
This document describes the design process for creating a dynamic adult airway management trainer (DAAMT) with interchangeable normal and inflamed tongues. The team tested various tongue materials and compositions to select ones that most accurately replicated tongue movement, size, shape and compressibility. User testing was conducted comparing the model to Laerdal's simulator and evaluating intubation difficulty levels and time to interchange tongues. The final design included silicone tongues of varying sizes mounted on interchangeable plates to allow realistic movement and withstanding of intubation forces while accommodating different inflammation levels.






















![Temporization or provisional restoration copy [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/temporizationorprovisionalrestoration-copyautosaved-211029145754-thumbnail.jpg?width=640&height=640&fit=bounds)









































