- A 23-year-old woman at 38 weeks gestation presents with complaints of diminished fetal movement for 2 days. Diminished fetal movement can indicate impending fetal death so this is a significant concern. The next step should be to assess the fetus, such as with a non-stress test (NST).
- Fetal monitoring aims to prevent fetal death and avoid unnecessary interventions. Methods include daily fetal movement counts (DFMC), NST, contraction stress tests (CST), biophysical profiles, and Doppler velocimetry. Interpretation depends on gestational age and fetal viability.
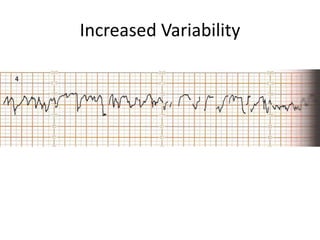
- An NST evaluates fetal condition by looking for fetal heart rate accelerations in response to movement. For gestations over