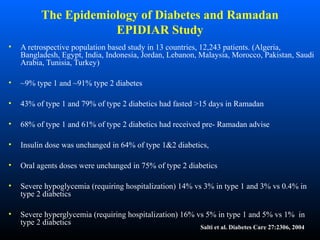
This document discusses health issues related to fasting during Ramadan. It covers effects on glucose metabolism, weight, cholesterol, uric acid, and diabetes. Fasting can cause hypoglycemia in diabetics and weight loss benefits those who are overweight. It also discusses adaptations to fasting, dietary recommendations during Ramadan, and effects on pregnancy, cardiovascular health, headaches, and other medical conditions. Exemptions from fasting are outlined for certain high-risk groups.