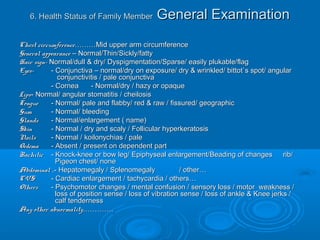
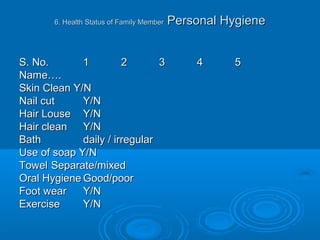
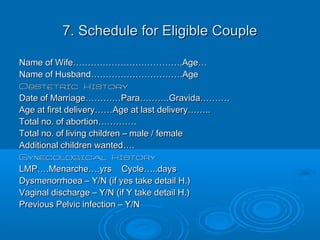
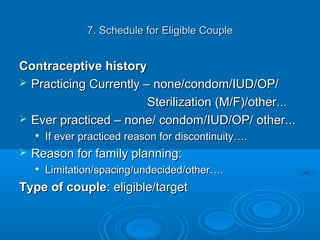
The document provides details about conducting a family survey. The objectives are to familiarize students with community health concepts, understand environmental and family factors influencing health, and provide comprehensive healthcare to families. The survey collects general family information, child health records, assessments of the physical, biological and meteorological environment, nutritional status, health records of family members, schedules for eligible couples and antenatal cases. Comprehensive information is gathered to understand health issues facing the family and provide appropriate recommendations.