OUTLINE
Contraception methods (Casey,2024)
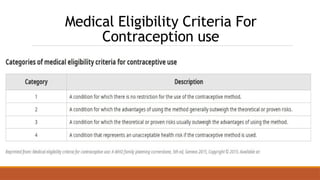
Medical eligibility criteria for conception use
Contraception counselling (Dehlendorf, 2025)
Emergency contraception (Turok, 2025)
3.
Introduction
•What is familyplanning?
-Controlling the number and spacing of children
•Why family planning? (WHO, 2015)
-Avoiding risky pregnancies
-Controlled distribution of food and resources to children
-Delayed first pregnancy for young people
4.
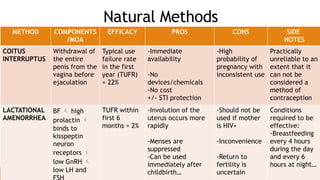
Natural Methods
METHOD COMPONENTS
/MOA
EFFICACYPROS CONS SIDE
NOTES
COITUS
INTERRUPTUS
Withdrawal of
the entire
penis from the
vagina before
ejaculation
Typical use
failure rate
in the first
year (TUFR)
= 22%
-Immediate
availability
-No
devices/chemicals
-No cost
+/- STI protection
-High
probability of
pregnancy with
inconsistent use
Practically
unreliable to an
extent that it
can not be
considered a
method of
contraception
LACTATIONAL
AMENORRHEA
BF high
prolactin
binds to
kisspeptin
neuron
receptors
low GnRH
low LH and
FSH
TUFR within
first 6
months = 2%
-Involution of the
uterus occurs more
rapidly
-Menses are
suppressed
-Can be used
immediately after
childbirth…
-Should not be
used if mother
is HIV+
-Inconvenience
-Return to
fertility is
uncertain
Conditions
required to be
effective:
-Breastfeeding
every 4 hours
during the day
and every 6
hours at night…
5.
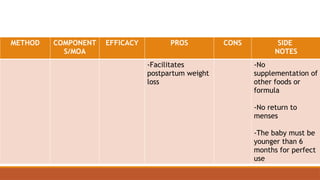
METHOD COMPONENT
S/MOA
EFFICACY PROSCONS SIDE
NOTES
-Facilitates
postpartum weight
loss
-No
supplementation of
other foods or
formula
-No return to
menses
-The baby must be
younger than 6
months for perfect
use
6.
Calendar Method
3 principleassumptions:
(1) A human ovum is capable of fertilization only for
approximately 24 hours after ovulation
(2) Spermatozoa can retain their fertilizing ability for 48h after
coitus
(3) Ovulation usually occurs 12-16 days before the onset of the
subsequent menses
7.
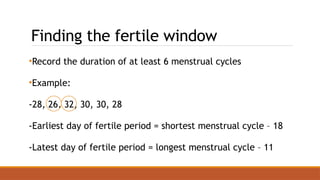
Finding the fertilewindow
•Record the duration of at least 6 menstrual cycles
•Example:
-28, 26, 32, 30, 30, 28
-Earliest day of fertile period = shortest menstrual cycle – 18
-Latest day of fertile period = longest menstrual cycle – 11
8.
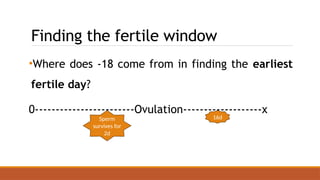
Finding the fertilewindow
•Where does -18 come from in finding the earliest
fertile day?
0------------------------Ovulation-------------------x
16d
Sperm
survives for
2d
9.
Finding the fertilewindow
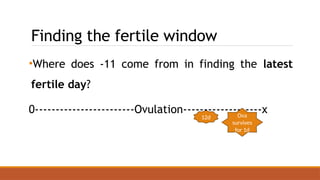
•Where does -11 come from in finding the latest
fertile day?
0------------------------Ovulation-------------------x
12d Ova
survives
for 1d
10.
Finding the fertilewindow
Worked example:
if the shortest cycle is 26 days and the longest is 32 days:
First fertile day: 26 - 18 = Day 8
Last fertile day: 32 - 11 = Day 21
Thus, days 8 through 21 are considered fertile.
11.
Standard Day Method
Thestandard day method assume a menstrual cycle
of 26-32d and gives a fertile period from day 8-19
Cyclic beads are used as a tool for this method
12.
Cervical Mucus Method
•Highestrogen prior to ovulation more elastic and
copious mucus until a peak day is reached ovulation
occurs then progesterone increases mucus becomes
scant and dry until next menses
•Intercourse is allowed 4 days after the maximal
cervical mucus until menstruation.
13.
Symptothermal Method
•In follicularphase, basal body temperature is relatively
low
•In luteal phase there is high progesterone which binds
to its receptors in the anterior hypothalamus
increased production of NE and serotonin increased
metabolic rate heat production
14.
Symptothermal Method
•This temperaturerise typically ranges between 0.2 and
0.5°C.
•The increase begins 1 to 2 days following ovulation and
aligns with the rising progesterone levels.
• Intercourse may be resumed three days after the
temperature elevation begins.
15.
Areas To ConsiderFor Natural Methods
•Efficacy TUFR = 25%
•Advantages
-No adverse effects
-No cost
-May be the only method acceptable to couples for cultural or
religious reasons
16.
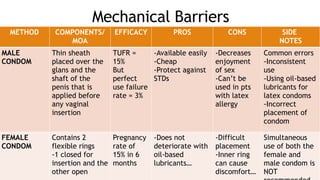
Mechanical Barriers
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
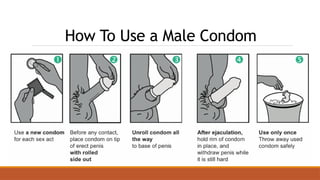
MALE
CONDOM
Thin sheath
placed over the
glans and the
shaft of the
penis that is
applied before
any vaginal
insertion
TUFR =
15%
But
perfect
use failure
rate = 3%
-Available easily
-Cheap
-Protect against
STDs
-Decreases
enjoyment
of sex
-Can’t be
used in pts
with latex
allergy
Common errors
-Inconsistent
use
-Using oil-based
lubricants for
latex condoms
-Incorrect
placement of
condom
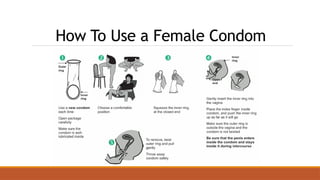
FEMALE
CONDOM
Contains 2
flexible rings
-1 closed for
insertion and the
other open
Pregnancy
rate of
15% in 6
months
-Does not
deteriorate with
oil-based
lubricants…
-Difficult
placement
-Inner ring
can cause
discomfort…
Simultaneous
use of both the
female and
male condom is
NOT
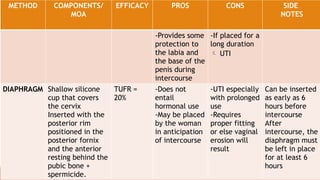
17.
METHOD COMPONENTS/
MOA
EFFICACY PROSCONS SIDE
NOTES
-Provides some
protection to
the labia and
the base of the
penis during
intercourse
-If placed for a
long duration
UTI
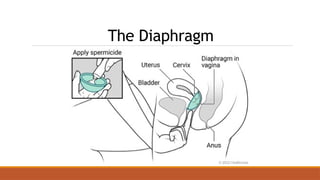
DIAPHRAGM Shallow silicone
cup that covers
the cervix
Inserted with the
posterior rim
positioned in the
posterior fornix
and the anterior
resting behind the
pubic bone +
spermicide.
TUFR =
20%
-Does not
entail
hormonal use
-May be placed
by the woman
in anticipation
of intercourse
-UTI especially
with prolonged
use
-Requires
proper fitting
or else vaginal
erosion will
result
Can be inserted
as early as 6
hours before
intercourse
After
intercourse, the
diaphragm must
be left in place
for at least 6
hours
Spermicidal Agents
•Consist ofa base (vaginal foams, suppositories, jellies,
films, foaming tablets, and creams) combined with
either nonoxynol-9 (toxic to lactobacilli as well) or
octoxynol = surfactant destroys sperm cell membranes
•Must be applied into the vagina prior to each coital act
22.
Spermicidal Agents
•Efficacy TUFR= 26%
•Advantages
-Easy to apply
-Additional lubricant function
•Disadvantages
-STI risk including HIV disrupts normal vaginal epithelium
Hormonal Contraceptives
•Mechanism ofaction
-Estrogen negative feedback on HPA decreased GnRH
decreased FSH and LH suppressed follicle
development and inhibited ovulation
-Progesterone as above + thickens cervical mucus +
altered tubal motility + endometrial atrophy
25.
Hormonal Contraceptives
•Mechanism ofside/adverse effects
Estrogen
-Slowed GI motility + stimulates CTZ nausea and
vomiting
-Alters serotonin and CGRP levels in neurons migraine
26.
Hormonal Contraceptives
-Stimulates hepaticproduction of angiotensinogen
increased RAAS activity vasoconstriction +
salt and water retention hypertension
-Alterations in fat metabolism and appetite
weight gain
27.
Hormonal Contraceptives
-High hepaticestrogen concentration increases
synthesis of procoagulants prothrombotic state
-Increases cholesterol synthesis + decreased bile acid
secretion + reduced emptying gallstones
-Binds to ERs in breast/liver stimulates cell division
mutation risk breast cancer/hepatic adenoma
Hormonal Contraceptives
-Stimulate cellproliferation and fluid accumulation in the
breast tissue breast fullness/tenderness
-Binds to androgen receptors in SCT increased sebum
production acne
-Asynchronous and unstable endometrial lining
menstrual irregularities
30.
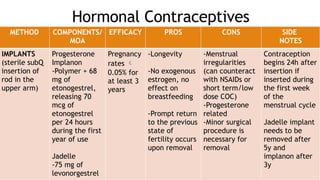
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
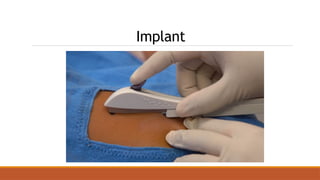
IMPLANTS
(sterile subQ
insertion of
rod in the
upper arm)
Progesterone
Implanon
-Polymer + 68
mg of
etonogestrel,
releasing 70
mcg of
etonogestrel
per 24 hours
during the first
year of use
Jadelle
-75 mg of
levonorgestrel
Pregnancy
rates
0.05% for
at least 3
years
-Longevity
-No exogenous
estrogen, no
effect on
breastfeeding
-Prompt return
to the previous
state of
fertility occurs
upon removal
-Menstrual
irregularities
(can counteract
with NSAIDs or
short term/low
dose COC)
-Progesterone
related
-Minor surgical
procedure is
necessary for
removal
Contraception
begins 24h after
insertion if
inserted during
the first week
of the
menstrual cycle
Jadelle implant
needs to be
removed after
5y and
implanon after
3y
31.
Implant
-Stimulate cell proliferationand fluid accumulation in the
breast tissue breast fullness/tenderness
-Binds to androgen receptors in SCT increased sebum
production acne
-Asynchronous and unstable endometrial lining menstrual
irregularities
32.
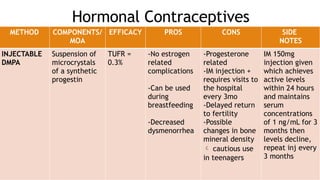
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
INJECTABLE
DMPA
Suspension of
microcrystals
of a synthetic
progestin
TUFR =
0.3%
-No estrogen
related
complications
-Can be used
during
breastfeeding
-Decreased
dysmenorrhea
-Progesterone
related
-IM injection +
requires visits to
the hospital
every 3mo
-Delayed return
to fertility
-Possible
changes in bone
mineral density
cautious use
in teenagers
IM 150mg
injection given
which achieves
active levels
within 24 hours
and maintains
serum
concentrations
of 1 ng/mL for 3
months then
levels decline,
repeat inj every
3 months
33.
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
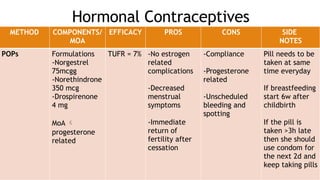
POPs Formulations
-Norgestrel
75mcgg
-Norethindrone
350 mcg
-Drospirenone
4 mg
MoA
progesterone
related
TUFR = 7% -No estrogen
related
complications
-Decreased
menstrual
symptoms
-Immediate
return of
fertility after
cessation
-Compliance
-Progesterone
related
-Unscheduled
bleeding and
spotting
Pill needs to be
taken at same
time everyday
If breastfeeding
start 6w after
childbirth
If the pill is
taken >3h late
then she should
use condom for
the next 2d and
keep taking pills
34.
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
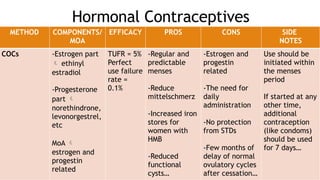
COCs -Estrogen part
ethinyl
estradiol
-Progesterone
part
norethindrone,
levonorgestrel,
etc
MoA
estrogen and
progestin
related
TUFR = 5%
Perfect
use failure
rate =
0.1%
-Regular and
predictable
menses
-Reduce
mittelschmerz
-Increased iron
stores for
women with
HMB
-Reduced
functional
cysts…
-Estrogen and
progestin
related
-The need for
daily
administration
-No protection
from STDs
-Few months of
delay of normal
ovulatory cycles
after cessation…
Use should be
initiated within
the menses
period
If started at any
other time,
additional
contraception
(like condoms)
should be used
for 7 days…
35.
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
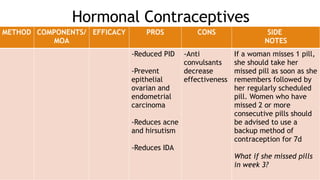
-Reduced PID
-Prevent
epithelial
ovarian and
endometrial
carcinoma
-Reduces acne
and hirsutism
-Reduces IDA
-Anti
convulsants
decrease
effectiveness
If a woman misses 1 pill,
she should take her
missed pill as soon as she
remembers followed by
her regularly scheduled
pill. Women who have
missed 2 or more
consecutive pills should
be advised to use a
backup method of
contraception for 7d
What if she missed pills
in week 3?
36.
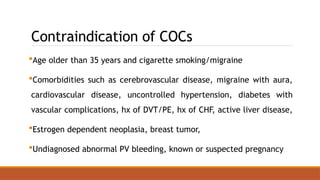
Contraindication of COCs
Ageolder than 35 years and cigarette smoking/migraine
Comorbidities such as cerebrovascular disease, migraine with aura,
cardiovascular disease, uncontrolled hypertension, diabetes with
vascular complications, hx of DVT/PE, hx of CHF, active liver disease,
Estrogen dependent neoplasia, breast tumor,
Undiagnosed abnormal PV bleeding, known or suspected pregnancy
37.
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
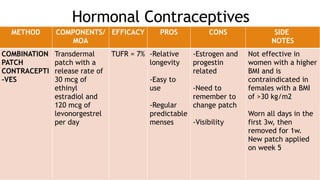
COMBINATION
PATCH
CONTRACEPTI
-VES
Transdermal
patch with a
release rate of
30 mcg of
ethinyl
estradiol and
120 mcg of
levonorgestrel
per day
TUFR = 7% -Relative
longevity
-Easy to
use
-Regular
predictable
menses
-Estrogen and
progestin
related
-Need to
remember to
change patch
-Visibility
Not effective in
women with a higher
BMI and is
contraindicated in
females with a BMI
of >30 kg/m2
Worn all days in the
first 3w, then
removed for 1w.
New patch applied
on week 5
38.
Hormonal Contraceptives
METHOD COMPONENTS/
MOA
EFFICACYPROS CONS SIDE
NOTES
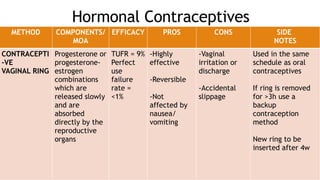
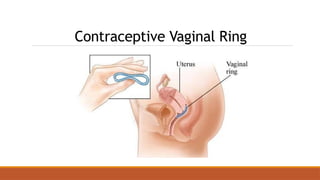
CONTRACEPTI
-VE
VAGINAL RING
Progesterone or
progesterone-
estrogen
combinations
which are
released slowly
and are
absorbed
directly by the
reproductive
organs
TUFR = 9%
Perfect
use
failure
rate =
<1%
-Highly
effective
-Reversible
-Not
affected by
nausea/
vomiting
-Vaginal
irritation or
discharge
-Accidental
slippage
Used in the same
schedule as oral
contraceptives
If ring is removed
for >3h use a
backup
contraception
method
New ring to be
inserted after 4w
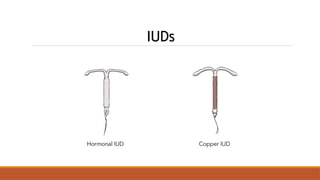
IUDs
METHOD COMPONENTS/
MOA
EFFICACY PROSCONS SIDE
NOTES
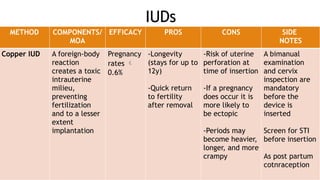
Copper IUD A foreign-body
reaction
creates a toxic
intrauterine
milieu,
preventing
fertilization
and to a lesser
extent
implantation
Pregnancy
rates
0.6%
-Longevity
(stays for up to
12y)
-Quick return
to fertility
after removal
-Risk of uterine
perforation at
time of insertion
-If a pregnancy
does occur it is
more likely to
be ectopic
-Periods may
become heavier,
longer, and more
crampy
A bimanual
examination
and cervix
inspection are
mandatory
before the
device is
inserted
Screen for STI
before insertion
As post partum
cotnraception
41.
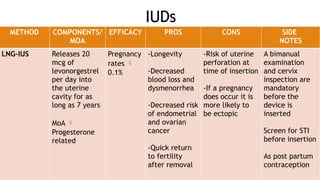
IUDs
METHOD COMPONENTS/
MOA
EFFICACY PROSCONS SIDE
NOTES
LNG-IUS Releases 20
mcg of
levonorgestrel
per day into
the uterine
cavity for as
long as 7 years
MoA
Progesterone
related
Pregnancy
rates
0.1%
-Longevity
-Decreased
blood loss and
dysmenorrhea
-Decreased risk
of endometrial
and ovarian
cancer
-Quick return
to fertility
after removal
-Risk of uterine
perforation at
time of insertion
-If a pregnancy
does occur it is
more likely to
be ectopic
A bimanual
examination
and cervix
inspection are
mandatory
before the
device is
inserted
Screen for STI
before insertion
As post partum
contraception
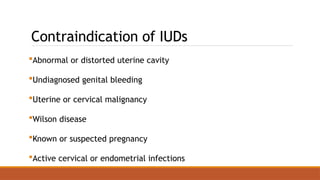
Contraindication of IUDs
Abnormalor distorted uterine cavity
Undiagnosed genital bleeding
Uterine or cervical malignancy
Wilson disease
Known or suspected pregnancy
Active cervical or endometrial infections
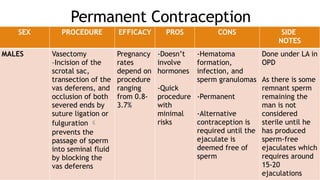
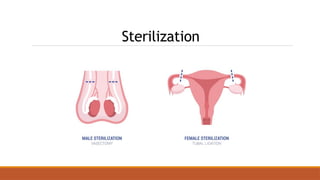
44.
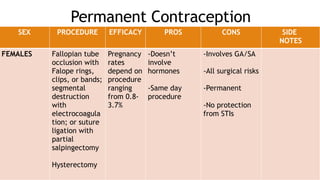
Permanent Contraception
SEX PROCEDUREEFFICACY PROS CONS SIDE
NOTES
FEMALES Fallopian tube
occlusion with
Falope rings,
clips, or bands;
segmental
destruction
with
electrocoagula
tion; or suture
ligation with
partial
salpingectomy
Hysterectomy
Pregnancy
rates
depend on
procedure
ranging
from 0.8-
3.7%
-Doesn’t
involve
hormones
-Same day
procedure
-Involves GA/SA
-All surgical risks
-Permanent
-No protection
from STIs
45.
Permanent Contraception
SEX PROCEDUREEFFICACY PROS CONS SIDE
NOTES
MALES Vasectomy
–Incision of the
scrotal sac,
transection of the
vas deferens, and
occlusion of both
severed ends by
suture ligation or
fulguration
prevents the
passage of sperm
into seminal fluid
by blocking the
vas deferens
Pregnancy
rates
depend on
procedure
ranging
from 0.8-
3.7%
-Doesn’t
involve
hormones
-Quick
procedure
with
minimal
risks
-Hematoma
formation,
infection, and
sperm granulomas
-Permanent
-Alternative
contraception is
required until the
ejaculate is
deemed free of
sperm
Done under LA in
OPD
As there is some
remnant sperm
remaining the
man is not
considered
sterile until he
has produced
sperm-free
ejaculates which
requires around
15-20
ejaculations
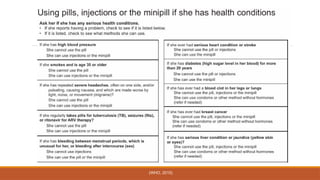
Contraception Counselling
•Shared decisionmaking
•Key points to consider:
-Desires pregnancy in the future?
-How important is pregnancy prevention now?
-Desired frequency of taking contraceptive method?
-Effect on menstrual bleeding and other side effects
-Non-contraceptive benefits
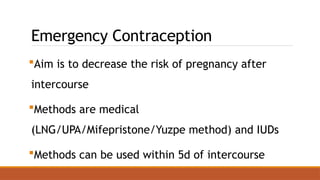
Emergency Contraception
Aim isto decrease the risk of pregnancy after
intercourse
Methods are medical
(LNG/UPA/Mifepristone/Yuzpe method) and IUDs
Methods can be used within 5d of intercourse
53.
References:
1. Casey, F.(2024) Contraception: Practice Essentials, Overview, Periodic Abstinence, Medscape.
Available at: https://emedicine.medscape.com/article/258507-overview (Accessed: 29 May
2025).
2. Dehlendorf, C. (2025) Contraception: Counseling and selection - UpToDate, Uptodate.
Available at: https://www.uptodate.com/contents/contraception-counseling-and-selection
(Accessed: 29 May 2025).
3. Turok, D. (2025) Emergency contraception - UpToDate, Uptodate. Available at:
https://www.uptodate.com/contents/emergency-contraception (Accessed: 29 May 2025).
4. WHO (2015) Medical eligibility criteria for contraceptive use. World Health Organization.
#16 Simultaneous use of both the female and male condom is not recommended because they may adhere to each other, leading to slippage or displacement of either device.










































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






