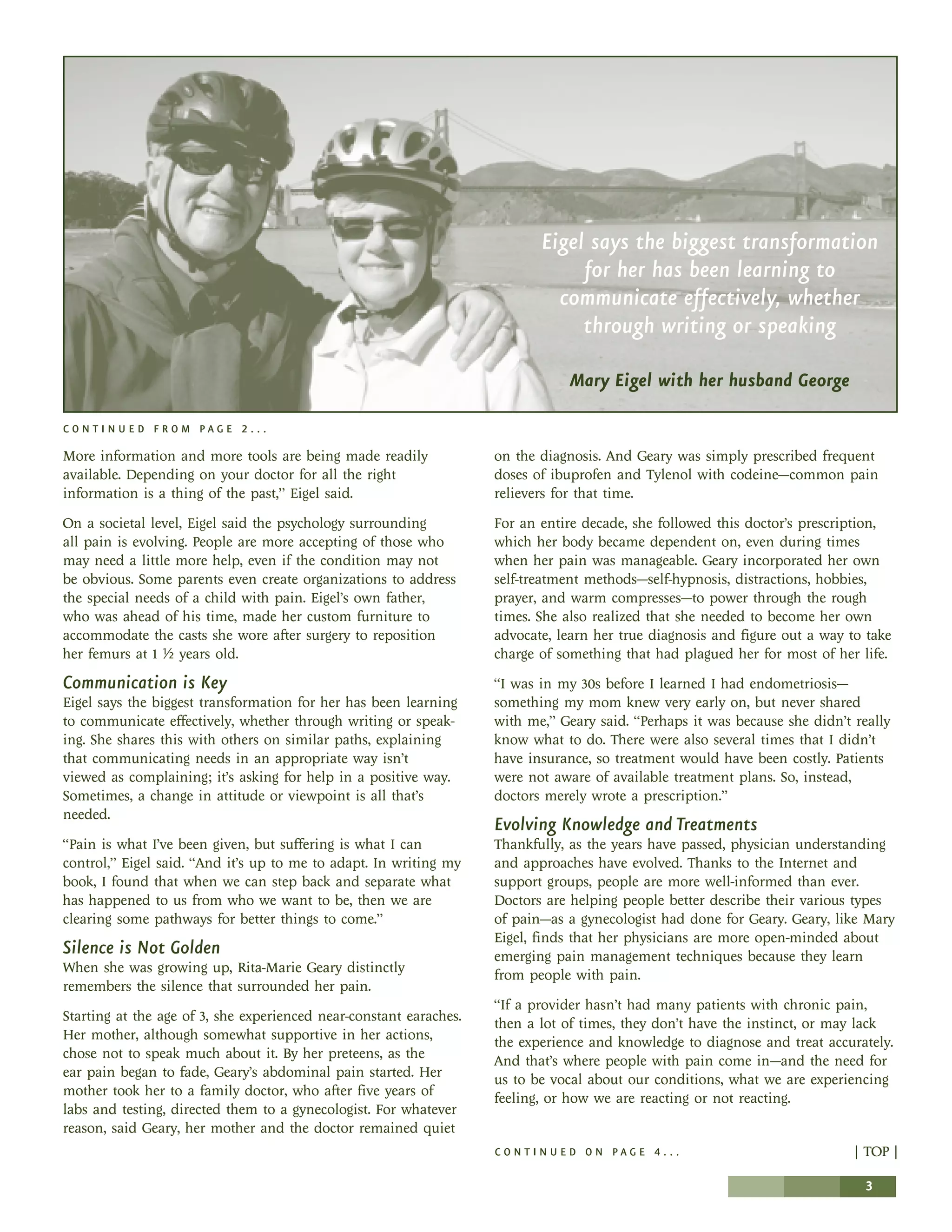
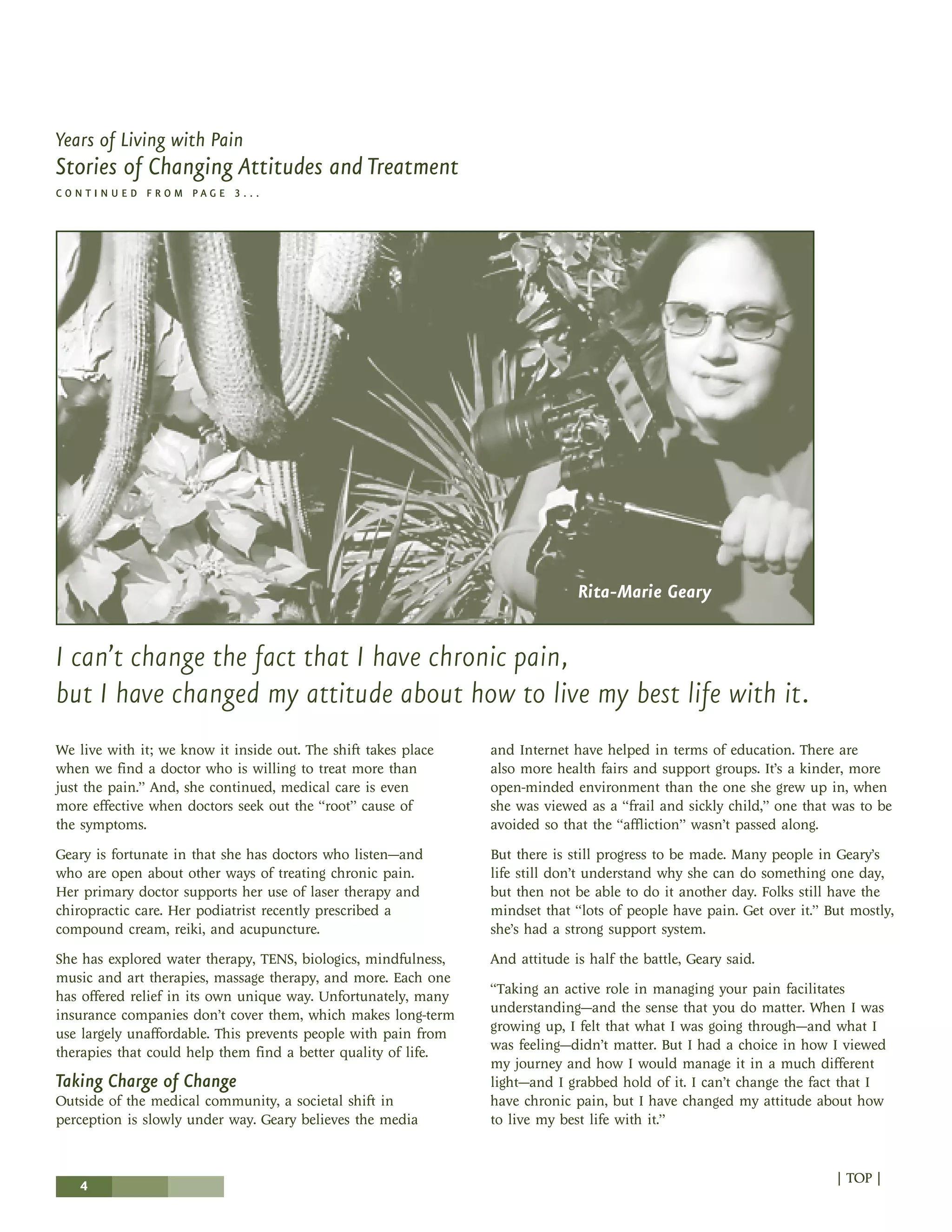
This document summarizes the stories of two women, Mary Eigel and Rita-Marie Geary, who have lived with chronic pain for most of their lives. It describes how attitudes and treatments for chronic pain have changed over time. Both women grew up in environments where pain was not discussed openly and treatment options were limited. However, they now have access to more support, information resources, and a wider range of medical and alternative treatment options. This has helped them to better manage their pain and lead more active lives.