Downloaded 77 times
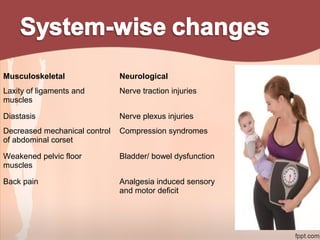
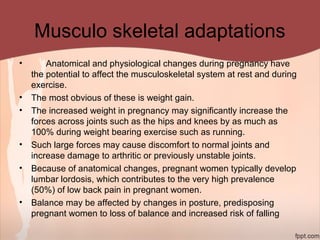
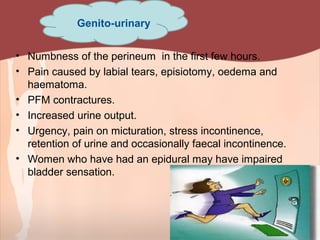
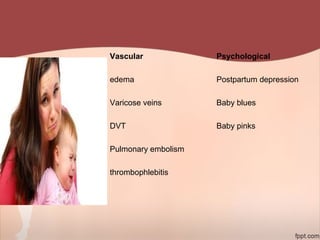
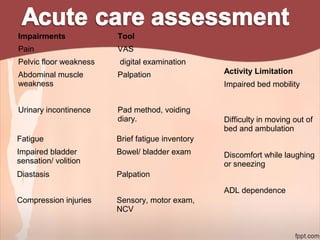






1. The document provides information on exercise prescription in the post-natal period, including detailing the post-partum phases, common musculoskeletal and neurological impairments, and appropriate physical therapy interventions. 2. Recommendations include encouraging early mobility to reduce risks, pelvic floor muscle exercises for pain relief and strengthening, and stabilization exercises progressed cautiously based on impairments. Modalities like ice, ultrasound, and electrical stimulation may assist with pain and dysfunction. 3. Physical therapy can effectively treat common post-natal issues like low back pain, pelvic girdle pain, and urinary incontinence when appropriate exercises and modalities are implemented safely based on each woman's individual presentation.