CONTENT
INTRODUCTION
DEFINITIONOF ETHICS
DENTAL ETHICS
HISTORY OF ETHICS
ETHICAL PRINCIPLES
UNETHICAL PRACTICES
SOME UN ETHICAL STUDIES IN HISTORY
UNETHICAL EXPERIMENTS IN TODAY'S MEDICINE
The IDA Code of Ethics
CONCLUSION
REFERENCE
4.
INTRODUCTION
The dental professionis a vocation in which knowledge
and skill is used for the service of others.
One of the characteristics of a profession is adherence to
a code of ethics. Being a health care provider it carrier
with it a responsibility to individual patients and society
confers on the professionals requires them to behave in an
ethical manner.
What is Ethics?
It’sa branch of philosophy concerned with the study of
those concepts that are used to evaluate human
activities, in particular the concepts of goodness and
obligation.
Dental ethics would mean moral duties and obligations
of the dentist towards his patients, professional
colleagues and to the society
8.
Definition of Ethics
Isdefined as "the science of the ideal human
character and behavior in situations where distinction
must be made between right and wrong, duty must
be followed and good interpersonal relations
maintained".
9.
DENTAL ETHICS
Dental ethicssimply means moral duties and
obligations of the dentists towards the
patients ,professional colleagues and to the
society.
These help support autonomy and self
determination , protect the vulnerable and
promote the welfare and equality of human
beings.
It deals with choices made by both clinicians
and patients
Macro-ethical principles
These area set of principles designed to
protect the human dignity, integrity, self
determination, confidentiality, rights and health
of populations and the people comprising
them.
13.
History of Ethics
AncientGreek ethics
Hippocratic oath is the first ethical standards given by
Hippocrates, the father of medicine, in the 4th century BC
It is perhaps the most widely known of Greek medical texts.
It requires a new physician to swear upon a number of
healing gods that he will uphold a number of professional
ethical standards. It also strongly binds the student to his
teacher and the greater community of physicians with
responsibilities similar to that of a family member
14.
Over thecenturies, it has been rewritten often in order
to suit the values of different cultures influenced by
Greek medicine.
Contrary to popular belief, the Hippocratic Oath is not
required by most modern medical schools, although
some have adopted modern versions that suit many in
the profession in the 21st
century
15.
Ancient Greek ethics
Socrates(5th century BC) –
Some problems are resolvable by data (e.g., geometry),
while others are moral issues (e.g., justice system)
Socrates, as portrayed in Plato's Republic, articulates the
greatest good as the transcendent "form of good itself".
The good, Socrates says, is like the sun. The sun gives light and
life to the earth, the good gives knowledge and virtue to the
intelligible world. It is the cause of goodness in people and
actions, and it also is the cause of existence and knowledge.
The pursuit of and love of the good itself (rather than any
particular good thing) Socrates thought was the chief aim of
education and (especially) of philosophy.
16.
Plato (5th-4th centuryBC)
Like most other ancient philosophers, Plato maintains
a virtue-based eudaemonistic conception of ethics.
That is to say, happiness or well-being (eudaimonia)
is the highest aim of moral thought and conduct,
and the virtues ( ‘excellence’) are the requisite skills
and dispositions needed to attain it.
Let’s give everyone the benefit of the doubt: ‘No
one knowingly harms himself or does evil things to
others because that would harm his soul.
17.
Aristotle (4th centuryBC)
Aristotle's ethics builds upon Plato's with important variations.
Aristotle's highest good was not the good itself but goodness
embodied in a flourishing human life.
His ethics are based on eudaimonia, variously translated as
"happiness," "prosperity," "flourishing," or "success."
A "great-souled" citizen who lives a life of virtue can expect to
achieve eudaimonia, which Aristotle argues is the highest good
for man.
Following Plato, Aristotle gives a significant role in moral life
the virtues, fixed habits of behavior that lead to good outcomes.
the main virtue are courage , justice, prudence and temperance
. The highest form of life is, however, purely intellectual activity.
18.
Kantian ethics
ImmanuelKant, in the 18th century, argued that right
and wrong are founded on duty, which issues
a Categorical Imperative to us, a command that, of
its nature, ought to be obeyed.
An action is only truly moral if done from a sense of
duty, and the most valuable thing is a human will that
has decided to act rightly. To decide what duty
requires, Kant proposes the principle
of universalizability correct moral rules are those
everyone could adopt.
19.
Natural law ethics
Inthe Middle Ages , Thomas Aquinas
developed a synthesis of Biblical and Aristotelian
ethics called natural law theory
According to which the nature of humans
determines what is right and wrong. For example,
murder is wrong because life is essential to humans
so depriving someone of it is inherently an evil.
Education is needed for humans, and is their right,
because their intellectual nature requires
developing
20.
Utilitarianism
In 19thcentury Britain, Jeremy Bentham and John Stuart
Mill advocated utilitarianism, the view that right actions are
those that are likely to result in the greatest happiness of the
greatest number. Utilitarianism remains popular in the twenty-
first century.
Both Kantianism and Utilitarianism provide ethical theories that
can support contemporary liberal political developments, and
associated enlightenment ways of conceiving of the
individual.
21.
In India, theDentist Act of 1948 was amended via
section 17A empowering the Dental Council of India to
prescribe standards of professional conduct & etiquette.
The Code of Ethics was framed by the Dental Council in
1975 & later notified by the Government of India as “
Dentists (code of ethics) Regulations 1976.
It is in force from August 1976.
22.
ETHICAL PRINCIPLES
To dono harm [ non-maleficence ]
To do good [ beneficence ]
Respect the person
Justice
Veracity or truthfulness
Confidentiality
23.
To do noharm [ non-maleficence ]
Considered to be the foundation of social morality.
Actions of the healthcare provider should not harm the
patients in anyway
24.
Iatrogenic diseases-doctorinduced illness.
• Use of unsterilized instruments
• Iatrogenic diseases (underfilling, overfilling etc)
• Doing procedures beyond his competency
The dentist, in cases where pain cannot be avoided, can make
attempts to minimize the pain. If feasible, the alternative of
minimal or no treatment can be presented to the patient.
Iatrogenic diseases-doctor induced illness.
• Use of unsterilized instruments
• Iatrogenic diseases (underfilling, overfilling etc)
• Doing procedures beyond his competency
The dentist, in cases where pain cannot be avoided, can make
attempts to minimize the pain. If feasible, the alternative of
minimal or no treatment can be presented to the patient.
25.
To do good[ beneficence ]
Prime responsibility of all dentists to benefit his patients as well as not to
inflict harm
The patient expects that the care provider will initiate beneficial
action & that there is an agreement between the doctor and the
patient that some good will result
In the process of treating a patient what has to be weighed are the
consequences of treatment Vs no treatment.
E.g. in questionable dental caries - the attempts should be
to maximize the benefits and minimize the harm.
26.
Respect the person
Itincorporates at least 2 fundamental
ethical considerations :
• Autonomy
• Informed Consent
27.
a) Autonomy
Thehealth care professionals respect the patient’s right to
make decisions concerning the treatment plan.
Patients should not be bystanders in their treatment , but
active participants
Dentist’s sometimes direct a patient towards a certain mode
of treatment by stressing certain advantages and not
mentioning the disadvantages
It is unethical to mislead or misinform patients.
28.
Dentists areoften trained in a paternalistic setting.
Paternalism is the principle of government as by a father, ie
a dictatorial “father knows best” attitude.
Paternalism in health care can take the form of withholding
information, restricting choices, or making the choice for the
patient.
We may be able to justify paternalistic laws as being in the
public’s interest, but we should recognize that these laws limit the
rights of a segment of the public because we judge that the laws
are in their “best interest”.
29.
b)Informed Consent
InformedConsent is the first stated and the largest principle of
the Nuremberg Code
The Nuremberg Code identifies 4 attributes of consent without
which consent cannot be considered valid.
Consent must be :
voluntary
Legally competent
Informed
comprehending
30.
Informed consent isa 2 step process.
i. Information is presented to the patient
by the doctor
ii. Patient satisfies himself/herself that
he/she understands & based upon this
understanding either agrees or refuses
to undergo treatment
31.
Informed Consent consistsof :
• A description of procedures to be carried out
• A description of any reasonably foreseeable
risks/discomforts to the subject
• A description of any benefits to the subject or to the
others which may reasonably br expected from the
treatment
• A disclosure of appropriate alternative procedures or
courses of treatment, if any, that might be
advantageous to the subject
32.
A statementdescribing the extent, if any, to which
confidentiality of records identifying the subject will be
maintained.
A statement that the patient has understood the
procedure and is willing to undergo the treatment
The signature of the patient and of a witness
33.
Justice
It isoften described as fairness / equal treatment,
giving to each her or his right or due .
Primary duty of the health professional is service
irrespective of class, creed etc
The principal of justice calls for an obligation to
protect the weak and to ensure equity in rights and
benefit, both for groups and for individuals
34.
Veracity or truthfulness
The patient – doctor relationship is based on
trust.
Lying shows disrespect to the patient and
threatens relationship
It is a principle that one would expect to go
unquestioned, yet many health care
professionals practice in a less than truthful way
35.
Confidentiality
Patient havethe right to expect that all
communications and records pertaining to their care
will be treated as confidential.
It is very natural to want to gossip about a patient,
particularly if it is someone famous or possibly a
neighbour ,but to do so that would break a bond of
trust between the dental professional and the
patient.
36.
WHY CODE OFMEDICAL AND DENTAL ETHICS?
Professions adopt ethical standards because that is part
of the professional charge.
A patient’s trust in a professional comes in part from the
expectation that the professional’s behaviour is
governed by norms prescribed by the group.
It is also a public expectation that ethical standards be
developed and enforced by any profession, a
requirement that comes with the privilege of self-
regulation.
37.
A systematicbody of rules is needed “in order that dignity and
honour of the dental profession may be upheld, its standard
exalted, its sphere of usefulness extended and the
advancement of dental sciences promoted and that the
members of the dental association may understand clearly their
duties and obligations to the dental profession, to their patients,
and to the community at large” (Indian Dental Association-
Constitution, bylaws and code of ethics, 1988).
38.
EHICAL RULES FORDENTISTS
[given by DCI]
Duties of dentist towards patients
Duties of dentists towards one
another
Duties of dentists towards the public
39.
DUTIES OF DENTISTTOWARDS PATIENTS
Dentists should be courteous, sympathetic, friendly and
helpful.
Observe punctuality in fulfilling his appointments.
He should establish a well merited reputation for
professional ability and fidelity.
Should not permit considerations of religion, nationality,
race, party politics or social
Information of a personal nature which may be learned
about or directly from a patient in the course of dental
practice should be kept in the utmost confidence. It is
also the obligation of the dentist to see that his auxiliary
staff observe this rule.
40.
Duties of dentiststowards one another
Every dentist should cherish a proper pride in his/her
colleagues and should not disparage them either by act or
word
A dentist called upon in any emergency to treat the patient
of another dentist, should, when the emergency is provided
for, retire in favour of the regular dentist but shall entitled to
charge the patient for his services
41.
When thedentist is entrusted with the care of the patient
of another, during sickness or absence, mutual
arrangements should be made regarding renumeration.
If a dentist is consulted by the patient of another dentist
and the former finds that the patient is suffering from
previous faulty treatment, it is his duty to institute correct
treatment at once with as little comments as possible
and in such manner as to avoid reflection on his
predecessor
42.
Duties of dentiststowards the public
Dentist should take leadership roles in the communities
on matters related to dental health
Practice by unregisteredpersons employed by the dentist
Dentist signed under his name and authority issuing any
certificate which is untrue, misleading or improper
Dentist advertising whether directly, or indirectly, for the
purpose of obtaining patients or promoting his own
professional advantage
Use of bogus diplomas etc.
Allowing commission
45.
Paying oraccepting commissions
Undercutting of charges in order to solicit patients
If planned treatment is beyond the dentist’s skill, the patient is
not referred to a consultant
In case of an emergency consultation during the temporary
absence of the patient’s dentist, temporary service is provided
and the patient is not sent back
If consulted, the dentist accepts charge of the case without
request of the referring dentist
1)The Tuskegee Study
The Tuskegee Study of Untreated Syphilis in the
Negro Male was an infamous and unethical clinical
study conducted between 1932 and 1972 by
the U.S. Public Health Service.
The purpose of this study was to observe the natural
history of untreated syphilis the African-American
men in the study were told they were receiving free
health care from the United States government
The Public Health Service started working on this
study in 1932 in collaboration with Tuskegee
University, a historically black college in Alabama
48.
ETHICAL PRINCIPLES NOTMET:
Respect for Human Dignity
Informed Consent
Respect for vulnerable persons
minimizing harm and maximizing benefit
Independence of research and conflicts of interest or
partiality must be explicit.
49.
2)The Monster Study(1939)
The Monster Study was a stuttering experiment on
22 orphan children in Davenport, Iowa, in 1939
conducted by Wendell Johnson at the University
of Iowa.
Johnson chose one of his graduate students, Mary
Tudor, to conduct the experiment and he
supervised her research.
After placing the children in control and
experimental groups, Tudor gave positive speech
therapy to half of the children, praising the fluency
of their speech, and negative speech therapy to
the other half, belittling the children for every
speech imperfection and telling them they were
stutterers.
50.
Many ofthe normal speaking orphan children who received
negative therapy in the experiment suffered negative
psychological effects and some retained speech problems
during the course of their life.
Dubbed “The Monster Study” by some of Johnson’s peers who
were horrified that he would experiment on orphan children to
prove a theory, the experiment was kept hidden for fear
Johnson’s reputation would be tarnished in the wake of human
experiments conducted by the Nazis during World War II. The
University of Iowa publicly apologized for the Monster Study in
2001.
51.
3) THE INHUMANNAZI EXPERIMENTS
Nazi human experimentation was a series
of medical experiments on large numbers
of prisoners, including children, by Nazi
Germany in its concentration camps in the
early to mid 1940s, during World War
II and the Holocaust.
Chief target populations
included Romani, Sinti, ethnic Poles, Soviet
POWs, disabled Germans, and Jews from
across Europe.
3) THE INHUMAN NAZI EXPERIMENTS
Nazi human experimentation was a series
of medical experiments on large numbers
of prisoners, including children, by Nazi
Germany in its concentration camps in the
early to mid 1940s, during World War
II and the Holocaust.
Chief target populations
included Romani, Sinti, ethnic Poles, Soviet
POWs, disabled Germans, and Jews from
across Europe.
52.
Nazi physicians andtheir assistants forced prisoners into
participating; they did not willingly volunteer and no
consent was given for the procedures.
Typically, the experiments resulted in
death, trauma, disfigurement or permanent disability, and
as such are considered examples of medical torture.
53.
ETHICAL PRINCIPLES NOTMET:
Respect for Human dignity
Informed Consent
Privacy
Respect for Vulnerable persons
Minimizing harm and maximizing benefit
54.
Experiments
Malaria experiments
Immunization experiments
Epidemic jaundice
Mustard gas experiments
Sulfonamide experiments
Experiments on twins
Bone, muscle, and nerve transplantation experiments
Experiments with poison
High altitude experiments
Blood coagulation experiments
55.
Malaria experiments
Fromabout February 1942 to about April 1945, experiments were
conducted at the Dachau concentration camp in order to
investigate immunization for treatment of malaria.
Healthy inmates were infected by mosquitoes or by injections of
extracts of the mucous glands of female mosquitoes. After
contracting the disease, the subjects were treated with various drugs
to test their relative efficiency.
Over 1,200 people were used in these experiments and more than
half died as a result. Other test subjects were left with permanent
disabilities
56.
Epidemic jaundice
FromJune 1943 till January 1945 at the concentration
camps, Sachsenhausen and Natzweiler,
experimentation with epidemic jaundice was
conducted.
The test subjects were injected with the disease in order
to discover new inoculations for the condition.
These tests were conducted for the benefit of the
German Armed Forces. Many suffered great pain in
these experiments
57.
Mustard gas experiments
At various times between September 1939 and April 1945, many
experiments were conducted at Sachsenhausen, Natzweiler,
and other camps to investigate the most effective treatment of
wounds caused by mustard gas.
Test subjects were deliberately exposed to mustard gas and
other vesicants (e.g. Lewisite) which inflicted severe chemical
burns.
The victims' wounds were then tested to find the most effective
treatment for the mustard gas burns
58.
Sulfonamide experiments
Fromabout July 1942 to about September 1943, experiments to investigate
the effectiveness of sulfonamide, a synthetic antimicrobial agent, were
conducted at Ravensbrück.
Wounds inflicted on the subjects were infected with bacteria such as
Streptococcus, Clostridium perfringens (a major causative agent in gas
gangrene) and Clostridium tetani, the causative agent in tetanus.
Circulation of blood was interrupted by tying off blood vessels at both ends
of the wound to create a condition similar to that of a battlefield wound.
Infection was aggravated by forcing wood shavings and ground glass into
the wounds. The infection was treated with sulfonamide and other drugs to
determine their effectiveness.
59.
Bone, muscle, andnerve transplantation
experiments
From about September 1942 to about December 1943
experiments were conducted at the Ravensbrück concentration
camp, for the benefit of the German Armed Forces, to study
bone, muscle, and nerve regeneration, and bone transplantation
from one person to another.
Sections of bones, muscles, and nerves were removed from the
subjects without use of anesthesia. As a result of these operations,
many victims suffered intense agony, mutilation, and permanent
disability
60.
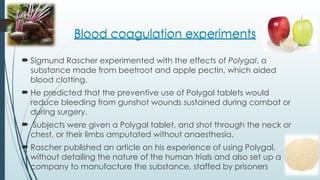
Blood coagulation experiments
Sigmund Rascher experimented with the effects of Polygal, a
substance made from beetroot and apple pectin, which aided
blood clotting.
He predicted that the preventive use of Polygal tablets would
reduce bleeding from gunshot wounds sustained during combat or
during surgery.
Subjects were given a Polygal tablet, and shot through the neck or
chest, or their limbs amputated without anaesthesia.
Rascher published an article on his experience of using Polygal,
without detailing the nature of the human trials and also set up a
company to manufacture the substance, staffed by prisoners
Blood coagulation experiments
62.
THE NUREMBERG CODE
It is a set of research ethical principles for human experimentation set
as a result of the Nuremberg trials at the end of 2nd
World War.
Specifically they were in response to the inhumane Nazi human
experimentation on un consenting prisoners during the 2nd
World War.
The code designed to protect the integrity of the research subject,
set out conditions for the ethical conduct of research involving
human subjects, emphasizing their voluntary consent to research.
63.
Voluntary informedconsent of the human subject is
absolutely essential . The duty & responsibility for ascertaining
the quality of the consent rests upon each individual who
initiates, directs or engages in the experiment. It is a personal
duty and responsibility which may not be delegated to
another with impunity
The experiment should be such as to yield fruitful results for
the good of society, unprocurable by other methods or
means of study, and not random and unnecessary in nature
64.
The experimentshould be designed and based on the
results of animal experimentation and a knowledge of
the natural history of the disease or other problem under
study that the anticipated results justify the
performance of the experiment
The experiment should be so conducted as to avoid all
unnecessary physical and mental suffering and injury
No experiment should be conducted where there is a
prior reason to believe that death or disabling injury will
occur.
65.
The degreeof risk to be taken should never exceed that
determined by the humanitarian importance of the problem
to be solved by the experiment
Proper preparations should be made and adequate facilities
provided to protect the experimental subject against even
remote possibilities of injury, disability or death.
The experiment should be conducted only by scientifically
qualified persons. The highest degree of skill and care should
be required through all stages of the experiment of those who
conduct or engage in the experiment
66.
During thecourse of the experiment the human subject
should be at liberty to bring the experiment to an end if
he has reached physical or mental state where
continuation of the experiment seems to him to be
impossible.
During the course of the experiment the scientist in
charge must be prepared to terminate the experiment
at any stage, if he has probable cause to believe, in the
exercise of the good faith, superior skill and careful
judgement required of him, that a continuation of the
experiment is likely to result in injury, disability or death to
the experimental subject.
67.
DECLARATION OF GENEVA
Was taken in the 2nd
General Assembly of World Medical
Association , Geneva 1948.
This oath seems to be a response to the atrocities committed by
doctors in Nazi Germany.
Notably this oath requires the physician to “not use (his) medical
knowledge contrary to the laws of humanity”
It is also called as Physician’s Pledge.
68.
At the timeof being admitted as a member of the medical profession:
The pledge reads :
I SOLEMNLY PLEDGE to dedicate my life to the service of humanity
THE HEALTH AND WELL-BEING OF MY PATIENT will be my first consideration
I WILL PRACTICE my profession with conscience and dignity.
I WILL RESPECT the secrets that are confined in me, even after the patient
has died.
69.
I WILLMAINTAIN by all means in my power , the honour and the
noble traditions of the medical profession.
MY COLLEAGUES will be my sisters and brothers.
THE HEALTH AND WELL-BEING OF MY PATIENT will be my first
consideration
I WILL MAINTAIN the utmost respect for human life.
I WILL NOT USE my medical knowledge to violate human rights and
civil liberties, even under threat;
I MAKE THESE PROMISES solemnly, freely and upon my honour
70.
WORLD MEDICAL ASSOCIATIONINTERNATIONAL CODE
OF MEDICAL ETHICS
Adopted in the 3rd
General Assembly of World Medical
Association , London October 1949
It states the duties of physician in general, to patients
and to colleagues
71.
DECLARATION OF HELSINSKI– 1964
Declaration of Helsinki is a set of ethical principles regarding human
experimentation developed for the medical community by the World
Medical Association (WMA).
It is widely regarded as the cornerstone document on human research
ethics.
The Declaration of Geneva of the WMA binds the physician with the
words, “The health of my patient will be my first consideration,” and the
International Code of Medical Ethics declares that, “A physician shall act
in the patient’s best interest when providing medical care.”
Research should be based on a thorough knowledge of the scientific
background
72.
Conducted bysuitably trained investigators using approved protocols,
While the primary purpose of medical research is to generate new
knowledge, this goal can never take precedence over the rights and
interests of individual research subjects.
Information regarding the study should be publicly available
Medical research should be conducted in a manner that minimizes
possible harm to the environment.
methods, but under certain circumstances a placebo or no treatment
group may be utilised
73.
Unethical experiments intoday's medicine
Updated January 22, 2019
Chinese scientist He Jiankui sent shockwaves
around the world last year with his claim that he
had modified twin babies' DNA before their birth.
and made the babies resistant to HIV.
Scientists from China and around the world spoke
out about the experiment, which many say was
unethical and not needed to prevent the virus. The
scientist had also been warned by peers not to go
down this path.
74.
Bombshell: Secret AmericanLaboratory Performs Deadly Human
Experiments in Caucasus’ Georgia
At a recent international meeting in Geneva,
representatives of Georgia’s breakaway region
of South Ossetia expressed concern that the
“Lugar Laboratory” in Tbilisi was contributing to
increased outbreaks of dangerous diseases in
South Ossetia
75.
However, Russia’sformer Chief Sanitary Inspector, Gennady
Onishchenko, suggested last year that the United States may be
spreading Zika-infected mosquitos in Georgia’s breakaway
Abkhazia region as a form of biological warfare against Russia
He told the BBC Russian Service that the discovery of Zika-infected
mosquitoes in Abkhazia’s Black Sea coast “worried” him “because
about 100 kilometers from the place where this mosquito now
lives, right near our borders, there is a military, microbiological
laboratory of the Army of the United States.”
76.
RECENT UN ETHICALTRIALS IN INDIA
The question whether all human clinical trials undertaken in India are
conducted ethically has been answered. The final report of the three-
member committee appointed by the central government to go into
the alleged irregularities in the conduct of the human papilloma virus
(HPV) vaccine trial reveals gross ethical violations.
The trial, suspended since March 2010, was carried out by the
Program for Appropriate Technology and Health(PATH), an NGO, in
collaboration with the Andhra Pradesh and Gujarat governments and
the Indian Council of Medical Research.
It was conducted on nearly 23,500 girls in the 10-14 years age group
in Khammam district (Andhra Pradesh) and Vadodra (Gujarat). The
“casual approach,” which saw the informed consent forms, the most
sacrosanct trial documents, being filled “very carelessly” with
“incomplete and probably inaccurate” information is shocking.
77.
In AndhraPradesh, nearly 2,800 consent forms were signed by a
hostel warden or headmaster, as the ‘guardian'. Since students
have “reduced autonomy,” the fact that teachers played a
“primary role” in explaining and “obtaining consent” meant that the
consent was obtained under duress, in a legally untenable way
The trial came under scrutiny following a public outcry over the
death of seven children. Although the cause of the deaths was
found to be unrelated to vaccination, the incident revealed a total
failure of the mechanism to monitor the ‘volunteers' for both serious
and non-serious adverse events following vaccination. There was a
five-month delay in reporting a death, while two deaths in
Khammam district went unreported.
78.
The IDA Codeof Ethics
The IDA Code of Ethics is a comprehensive directive on the ethical
codes of conduct an IDA dentist member is expected to follow.
The IDA code of ethics has been formulated keeping in mind the
DCI Code of Ethics i.e. Dentist’s Act amended in 2016 and adopted
from various international Dental Associations promoting high
standards of patient care matching global standards.
IDA strives to put India on the global map by holding its members to
a very high standard through the adoption of this Code of Ethics
These regulations may be called the Revised IDA Code of Ethics ,
2014.
79.
Codes of ethics
1.Declaration:
Everydentist who has been registered (either on Part A or Part B of the
State Dentists Register) shall, within a period of thirty days from the date
of commencement of these regulations, and every dentist who gets
himself registered after the commencement of these regulations shall,
within a period of thirty days from such registration, make, before the
Registrar of the State Dental Council, a declaration in the form set out for
the purpose in the Schedule to these regulations and shall agree to have
read, understood and thence to abide by the same.
80.
2. Duties andObligation of Dentists in General
4.1 Character of Dentist / Dental Surgeon
In view of the important role of a Dentist/ Dental Surgeon as a health
professional educated and trained in surgical and medical treatment of
diseases of the Oral cavity, he shall:
(4.1.1) Be mindful of the high character of his mission and the responsibilities he
holds in the discharge of his duties as an independent healthcare professional
and shall always remember that care of the patient and treatment of the
disease depends upon the skill and prompt attention shown by him and always
remembering that his personal reputation, professional ability and fidelity
remain his best recommendations;
(4.1.2) Treat the welfare of the patients as paramount to all other considerations
and shall conserve it to the utmost of his ability;
(4.1.3) Be courteous, sympathetic, friendly and helpful to, and always ready to
respond to the call of his patients, and that under all conditions his behavior
towards his patients and the public shall be polite and dignified.
81.
4.2 Maintaining goodClinical Practices:
The Principal objective of the Dental profession is to render service to
humanity with full respect for the dignity of profession and man. Dental
Surgeons should merit the confidence of patients entrusted to their care,
rendering to each a full measure of service and devotion
(4.2.1)The Dentist/ Dental Surgeon should practice methods of healing
founded on scientific basis and should not associate professionally with
anyone who violates this principle.
4.2.2) Membership in Dental and Medical Associations and Societies: For the
advancement of his/her profession, a Dental Surgeon should be
encouraged to affiliate with associations and societies of dental, oral and
allied medical professionals and play a proactive role in the promotion of
oral health in particular and health of an individual in general.
82.
4.3 Maintenance ofDental/Medical records:
(4.3.1) Every Dental surgeon shall maintain the relevant records pertaining to his
out- patients and inpatients (wherever applicable). These records must be
preserved for a minimum period of three years from the date of commencement
of the treatment in a format determined by the Council or accepted as a
standard mode of documentation.
(4.3.2) If any request is made for medical or dental records either by the
patients/authorized attendant or legal authorities involved, the same may be
issued to the competent authority within 72 hours after having obtained a valid
receipt for all documents.
4.3.3) A Registered Dental practitioner shall maintain a Register of Medical
Certificates giving full details of certificates issued.
83.
4.4 Display ofRegistration Numbers:
Every Dental practitioner shall display the registration number accorded to
him by the State Dental Council in his clinic and in all his prescriptions,
certificates and money receipts given to his patients.
4.5 Prescription of Drugs:
Every dental surgeon should take care to prescribe and administer drugs in a
responsible manner and ensure safe and rational use of drugs. He should as
far as possible, prescribe drugs in a generic form.
4.6 Highest Quality Assurance in patient care:
Every Dental practitioner should ensure quality treatment that does not
compromise the outcome of treatment.
All practitioners should be aware of unethical practices and practices by
unqualified persons.
84.
4.7 Exposure ofUnethical Conduct:
A Dental Surgeon should expose, without fear or favor, incompetent or
corrupt, dishonest or unethical conduct on the part of members of the
profession.
It is the responsibility of the dental surgeon to report to the competent
authorities’ instances of quackery and any kind of abuse including doctor-
patient sexual misconduct, misuse of fiduciary relationship, child abuse and
other social evils that may come to their attention.
4.8 Payment of Professional Services: The personal financial interests of a
dental surgeon should not conflict with the medical interests of patients. A
dental practitioner should announce his fees before rendering service and
not after the operation or treatment is under way .
85.
4.9 Observation ofStatutes:
The Dental Surgeon shall observe the laws of the country in regulating
the practice of his profession including the Dentists’ Act 1948 and its
amendments and shall also not assist others to evade such laws.
He should be cooperative in observance and enforcement of
sanitary laws and regulations in the interest of public health.
He should observe the provisions of the State Acts like Drugs and
Cosmetics Act, 1940; Pharmacy Act, 1948; Narcotic Drugs and
Psychotropic substances Act, 1985; Environmental Protection Act,
1986; Drugs and Magic Remedies (Objectionable Advertisement) Act,
1954; Persons with Disabilities (Equal Opportunities and Full
Participation) Act, 1995 and Bio-Medical Waste (Management and
Handling) Rules, 1998 and such other Acts, Rules, Regulations made
by the Central/State Governments or local Administrative Bodies or
any other relevant Act relating to the protection and promotion of
public health.
86.
4.10 Signing ProfessionalCertificates, Reports and other Documents:
A Registered Dental Surgeon involved independently in the
treatment of dental and oral surgical problems may be called
upon to sign certificates, notifications, reports etc. He is bound to
issue such certificates and to sign them. Documents relating to
disability, injury in the oral and maxillofacial region and deaths
occurring while under the care of such dental surgeons should be
signed by them in their professional capacity for subsequent use
in the courts or for administrative purposes etc.
Any registered dental surgeon who is shown to have signed or
given under his name and authority any such certificate,
notification, report or document of a similar character which is
untrue, misleading or improper, is liable to have his name deleted
from the Register.
87.
CONCLUSION
A professionconsists of a limited group of persons who have
acquired some special skill and are therefore able to perform
that function in society better than the average person.
A professional person is expected to have respect for human
beings, competence in his chosen field, integrity and a
primary concern with service rather than with prestige or
profit.
Ethical codes are the result of an attempt to direct the moral
consciousness of the members of the profession to its peculiar
problems.
Ethical codes are important in developing higher standards
of conduct, for they are based on the correct attitude and
the correct procedure.
88.
REFERENCE
Essentials ofPublic Health Dentistry – Soben Peter – 5th
Edition
Ethics and Research – Dr.JayakrishnanThavody
ETHICS IN DENTISTRY; Dr. Shika Swaroop Alva, Dr Shruthi Bhandary, Dr. Aftab
Damda International Journal of Current Research Vol. 9, Issue, 01,
pp.45692-45695, January, 2017
Code of ethics IDA






![ETHICAL PRINCIPLES
To do no harm [ non-maleficence ]
To do good [ beneficence ]
Respect the person
Justice
Veracity or truthfulness
Confidentiality](https://image.slidesharecdn.com/ethicsindentisrty-ppt-251203063042-5b4410bd/85/ethics-in-dentisrty-power-point-presentation-22-320.jpg)
![To do no harm [ non-maleficence ]
Considered to be the foundation of social morality.
Actions of the healthcare provider should not harm the
patients in anyway](https://image.slidesharecdn.com/ethicsindentisrty-ppt-251203063042-5b4410bd/85/ethics-in-dentisrty-power-point-presentation-23-320.jpg)
![To do good [ beneficence ]
Prime responsibility of all dentists to benefit his patients as well as not to
inflict harm
The patient expects that the care provider will initiate beneficial
action & that there is an agreement between the doctor and the
patient that some good will result
In the process of treating a patient what has to be weighed are the
consequences of treatment Vs no treatment.
E.g. in questionable dental caries - the attempts should be
to maximize the benefits and minimize the harm.](https://image.slidesharecdn.com/ethicsindentisrty-ppt-251203063042-5b4410bd/85/ethics-in-dentisrty-power-point-presentation-25-320.jpg)



![EHICAL RULES FOR DENTISTS
[given by DCI]
Duties of dentist towards patients
Duties of dentists towards one
another
Duties of dentists towards the public](https://image.slidesharecdn.com/ethicsindentisrty-ppt-251203063042-5b4410bd/85/ethics-in-dentisrty-power-point-presentation-38-320.jpg)